Department of Anaesthesiology and Critical Care Medicine, Estaing Hospital, University Hospital of Clermont-Ferrand, Clermont-Ferrand, France.
INSERM U1190, CHU Lille, Department of Critical Care Medicine, Roger Salengro Hospital, Univ. Lille, 59000, Lille, France.
Crit Care. 2020 Dec 2;24(1):672. doi: 10.1186/s13054-020-03402-7.
There is wide variability between intensivists in the decisions to forgo life-sustaining treatment (DFLST). Advance directives (ADs) allow patients to communicate their end-of-life wishes to physicians. We assessed whether ADs reduced variability in DFLSTs between intensivists.
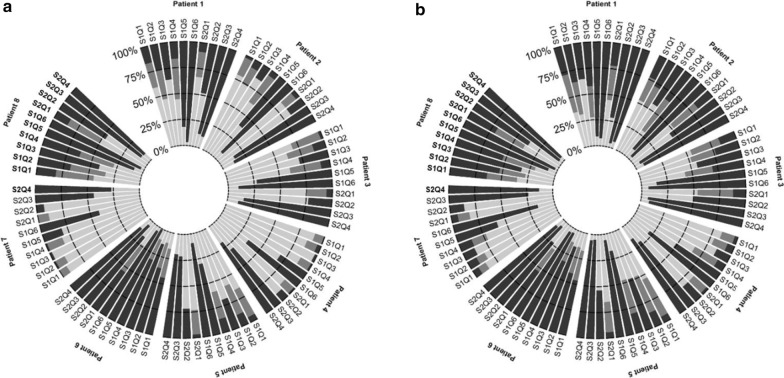
We conducted a multicenter, prospective, simulation study. Eight patients expressed their wishes in ADs after being informed about DFLSTs by an intensivist-investigator. The participating intensivists answered ten questions about the DFLSTs of each patient in two scenarios, referring to patients' characteristics without ADs (round 1) and then with (round 2). DFLST score ranged from 0 (no-DFLST) to 10 (DFLST for all questions). The main outcome was variability in DFLSTs between intensivists, expressed as relative standard deviation (RSD).
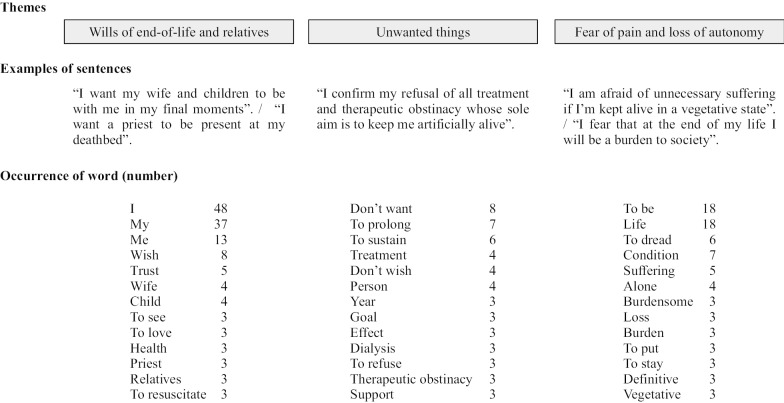
A total of 19,680 decisions made by 123 intensivists from 27 ICUs were analyzed. The DFLST score was higher with ADs than without (6.02 95% CI [5.85; 6.19] vs 4.92 95% CI [4.75; 5.10], p < 0.001). High inter-intensivist variability did not change with ADs (RSD: 0.56 (round 1) vs 0.46 (round 2), p = 0.84). Inter-intensivist agreement on DFLSTs was weak with ADs (intra-class correlation coefficient: 0.28). No factor associated with DFLSTs was identified. A qualitative analysis of ADs showed focus on end-of-life wills, unwanted things and fear of pain.
ADs increased the DFLST rate but did not reduce variability between the intensivists. In the decision-making process using ADs, the intensivist's decision took priority. Further research is needed to improve the matching of the physicians' decision with the patient's wishes. Trial registration ClinicalTrials.gov Identifier: NCT03013530. Registered 6 January 2017; https://clinicaltrials.gov/ct2/show/NCT03013530 .
在放弃生命维持治疗(DFLST)的决策方面,重症监护医生之间存在广泛的差异。预先指示(AD)允许患者将其临终意愿传达给医生。我们评估了 AD 是否减少了重症监护医生之间 DFLST 的变异性。
我们进行了一项多中心、前瞻性、模拟研究。8 名患者在一名重症监护医生研究员告知 DFLST 后,通过 AD 表达了他们的意愿。参与的重症监护医生在两种情况下回答了每个患者的 10 个 DFLST 问题,参考患者的特征,没有 AD(第 1 轮),然后是有 AD(第 2 轮)。DFLST 评分范围从 0(无 DFLST)到 10(所有问题的 DFLST)。主要结局是重症监护医生之间 DFLST 的变异性,用相对标准差(RSD)表示。
共分析了来自 27 个 ICU 的 123 名重症监护医生做出的 19680 项决策。有 AD 时 DFLST 评分高于无 AD(6.02,95%CI[5.85;6.19]比 4.92,95%CI[4.75;5.10],p<0.001)。有 AD 时,重症监护医生之间的高变异性没有改变(RSD:0.56(第 1 轮)比 0.46(第 2 轮),p=0.84)。有 AD 时,重症监护医生对 DFLST 的一致性较弱(组内相关系数:0.28)。未发现与 DFLST 相关的因素。对 AD 的定性分析表明,重点是临终意愿、不想要的事情和对疼痛的恐惧。
AD 增加了 DFLST 的比例,但没有减少重症监护医生之间的变异性。在使用 AD 的决策过程中,重症监护医生的决策优先。需要进一步研究以提高医生决策与患者意愿的匹配程度。
ClinicalTrials.gov 标识符:NCT03013530。注册于 2017 年 1 月 6 日;https://clinicaltrials.gov/ct2/show/NCT03013530。