Ciarkowski Claire E, Timbrook Tristan T, Kukhareva Polina V, Edholm Karli M, Hatton Nathan D, Hopkins Christy L, Thomas Frank, Sanford Matthew N, Igumnova Elena, Benefield Russell J, Kawamoto Kensaku, Spivak Emily S
Division of General Internal Medicine, Department of Internal Medicine, University of Utah School of Medicine, Salt Lake City, Utah, USA.
Department of Pharmacy, University of Utah, Salt Lake City, Utah, USA.
Open Forum Infect Dis. 2020 Oct 19;7(11):ofaa497. doi: 10.1093/ofid/ofaa497. eCollection 2020 Nov.
Evidence supports streamlined approaches for inpatients with community-acquired pneumonia (CAP) including early transition to oral antibiotics and shorter therapy. Uptake of these approaches is variable, and the best approaches to local implementation of infection-specific guidelines are unknown. Our objective was to evaluate the impact of a clinical decision support (CDS) tool linked with a clinical pathway on CAP care.
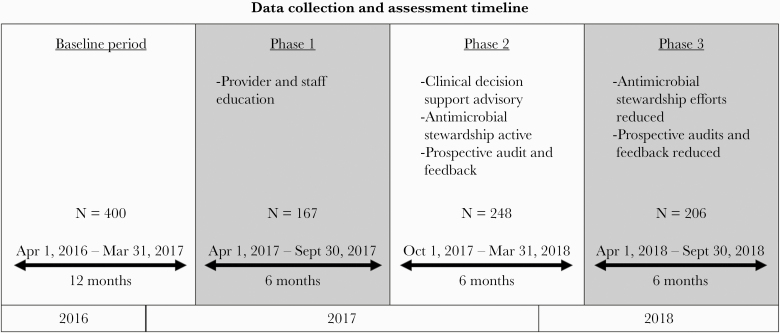
This is a retrospective, observational pre-post intervention study of inpatients with pneumonia admitted to a single academic medical center. Interventions were introduced in 3 sequential 6-month phases; Phase 1: education alone; Phase 2: education and a CDS-driven CAP pathway coupled with active antimicrobial stewardship and provider feedback; and Phase 3: education and a CDS-driven CAP pathway without active stewardship. The 12 months preceding the intervention were used as a baseline. Primary outcomes were length of intravenous antibiotic therapy and total length of antibiotic therapy. Clinical, process, and cost outcomes were also measured.
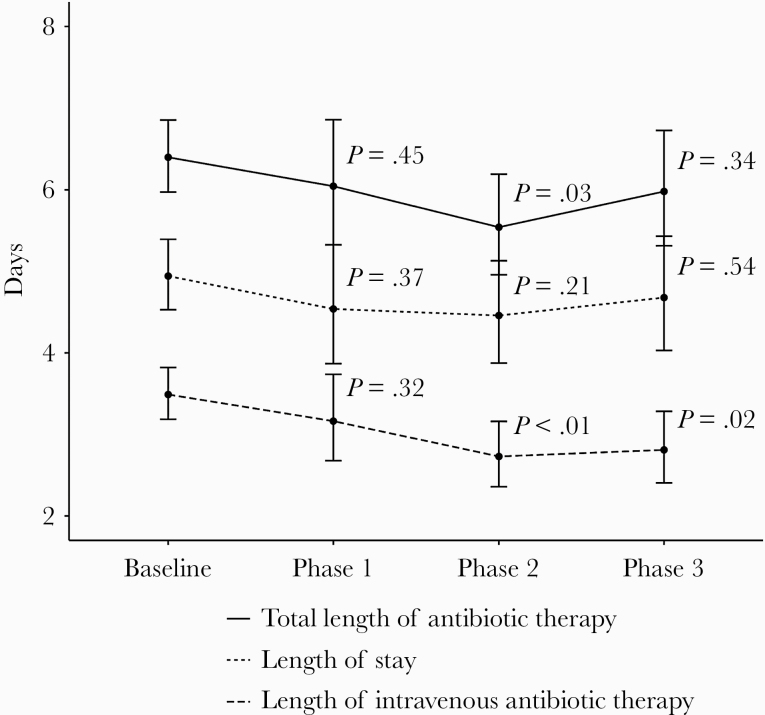
The study included 1021 visits. Phase 2 was associated with significantly lower length of intravenous and total antibiotic therapy, higher procalcitonin lab utilization, and a 20% cost reduction compared with baseline. Phase 3 was associated with significantly lower length of intravenous antibiotic therapy and higher procalcitonin lab utilization compared with baseline.
A CDS-driven CAP pathway supplemented by active antimicrobial stewardship review led to the most robust improvements in antibiotic use and decreased costs with similar clinical outcomes.
有证据支持对社区获得性肺炎(CAP)住院患者采用简化治疗方法,包括尽早转换为口服抗生素及缩短治疗疗程。这些方法的采用情况各不相同,且针对特定感染实施本地指南的最佳方法尚不清楚。我们的目标是评估与临床路径相关联的临床决策支持(CDS)工具对CAP治疗的影响。
这是一项对一所学术医疗中心收治的肺炎住院患者进行的回顾性观察性干预前后研究。干预分3个连续的6个月阶段实施;第1阶段:仅进行教育;第2阶段:教育以及由CDS驱动的CAP路径,同时开展积极的抗菌药物管理及向医疗服务提供者反馈;第3阶段:教育以及由CDS驱动的CAP路径,但不进行积极的管理。干预前的12个月用作基线。主要结局为静脉用抗生素治疗时长及抗生素治疗总时长。还对临床、过程及成本结局进行了测量。
该研究纳入了1021例就诊患者。与基线相比,第2阶段静脉用抗生素和抗生素治疗总时长显著缩短,降钙素原实验室检测的利用率更高,成本降低了20%。与基线相比,第3阶段静脉用抗生素治疗时长显著缩短,降钙素原实验室检测的利用率更高。
由CDS驱动的CAP路径辅以积极的抗菌药物管理审查,在抗生素使用方面带来了最显著的改善,降低了成本,且临床结局相似。