Division of General Internal Medicine, Department of Internal Medicine, University of Utah School of Medicine, Salt Lake City, Utah, USA.
Division of Health System Innovation & Research, Department of Population Health Science, University of Utah School of Medicine, Salt Lake City, Utah, USA.
Clin Infect Dis. 2022 Aug 31;75(3):460-467. doi: 10.1093/cid/ciab950.
Community-acquired pneumonia (CAP) is a common cause for hospitalization and antibiotic overuse. We aimed to improve antibiotic duration for CAP across 41 hospitals participating in the Michigan Hospital Medicine Safety Consortium (HMS).
This prospective collaborative quality initiative included patients hospitalized with uncomplicated CAP who qualified for a 5-day antibiotic duration. Between 23 February 2017 and 5 February 2020, HMS targeted appropriate 5-day antibiotic treatment through benchmarking, sharing best practices, and pay-for-performance incentives. Changes in outcomes, including appropriate receipt of 5 ± 1-day antibiotic treatment and 30-day postdischarge composite adverse events (ie, deaths, readmissions, urgent visits, and antibiotic-associated adverse events), were assessed over time (per 3-month quarter), using logistic regression and controlling for hospital clustering.
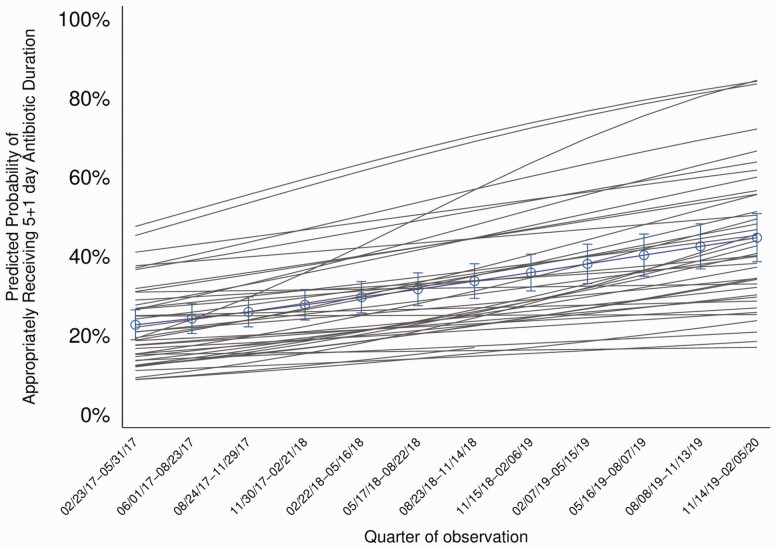
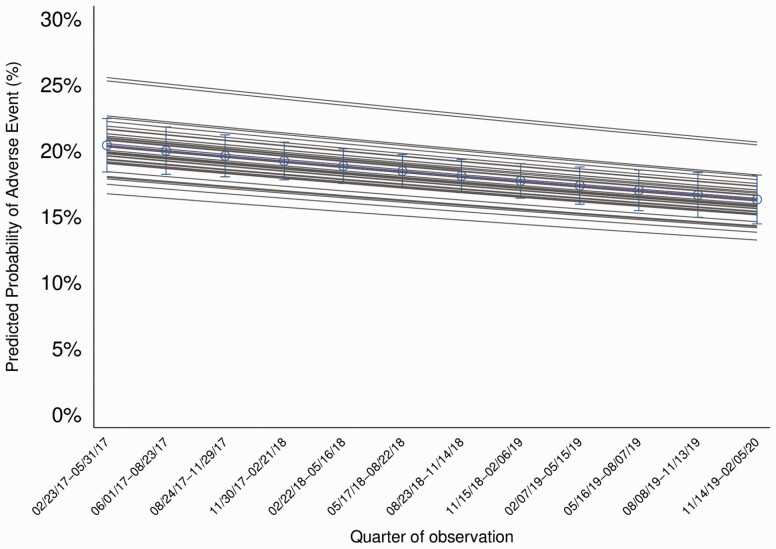
A total of 41 hospitals and 6553 patients were included. The percentage of patients treated with an appropriate 5 ± 1-day duration increased from 22.1% (predicted probability, 20.9% [95% confidence interval: 17.2%-25.0%]) to 45.9% (predicted probability, 43.9% [36.8%-51.2%]; adjusted odds ratio [aOR] per quarter, 1.10 [1.07-1.14]). Thirty-day composite adverse events occurred in 18.5% of patients (1166 of 6319) and decreased over time (aOR per quarter, 0.98 [95% confidence interval: .96-.99]) owing to a decrease in antibiotic-associated adverse events (aOR per quarter, 0.91 [.87-.95]).
Across diverse hospitals, HMS participation was associated with more appropriate use of short-course therapy and fewer adverse events in hospitalized patients with uncomplicated CAP. Establishment of national or regional collaborative quality initiatives with data collection and benchmarking, sharing of best practices, and pay-for-performance incentives may improve antibiotic use and outcomes for patients hospitalized with uncomplicated CAP.
社区获得性肺炎(CAP)是住院和抗生素过度使用的常见原因。我们旨在改善密歇根医院医学安全联盟(HMS)参与的 41 家医院的 CAP 抗生素使用疗程。
这项前瞻性协作质量计划包括因符合 5 天抗生素疗程标准而住院的无并发症 CAP 患者。在 2017 年 2 月 23 日至 2020 年 2 月 5 日期间,HMS 通过基准测试、分享最佳实践和基于绩效的激励措施,针对适当的 5 天抗生素治疗目标。使用逻辑回归并控制医院聚类,评估随着时间推移(每 3 个月季度)的结果变化,包括适当接受 5 ± 1 天抗生素治疗和 30 天出院后复合不良事件(即死亡、再入院、紧急就诊和抗生素相关不良事件)的情况。
共纳入 41 家医院和 6553 名患者。接受适当 5 ± 1 天疗程治疗的患者比例从 22.1%(预测概率,20.9%[95%置信区间:17.2%-25.0%])上升至 45.9%(预测概率,43.9%[36.8%-51.2%];每季度调整优势比[aOR],1.10[1.07-1.14])。30 天复合不良事件发生在 18.5%的患者(6319 例中有 1166 例),随着时间的推移而减少(每季度 aOR,0.98[95%置信区间:0.96-.99]),这归因于抗生素相关不良事件的减少(每季度 aOR,0.91[0.87-.95])。
在多样化的医院中,HMS 参与与住院治疗无并发症 CAP 患者更适当的短疗程治疗和更少的不良事件相关。建立具有数据收集和基准测试、分享最佳实践和基于绩效的激励措施的全国或地区合作质量计划可能会改善住院治疗无并发症 CAP 患者的抗生素使用和结局。