Department of Gynecology, Chiba University Graduate School of Medicine, 1-8-1, Inohana, Chuou-ku, Chiba city, Chiba, 2608677, Japan.
Sci Rep. 2020 Dec 4;10(1):21307. doi: 10.1038/s41598-020-78296-0.
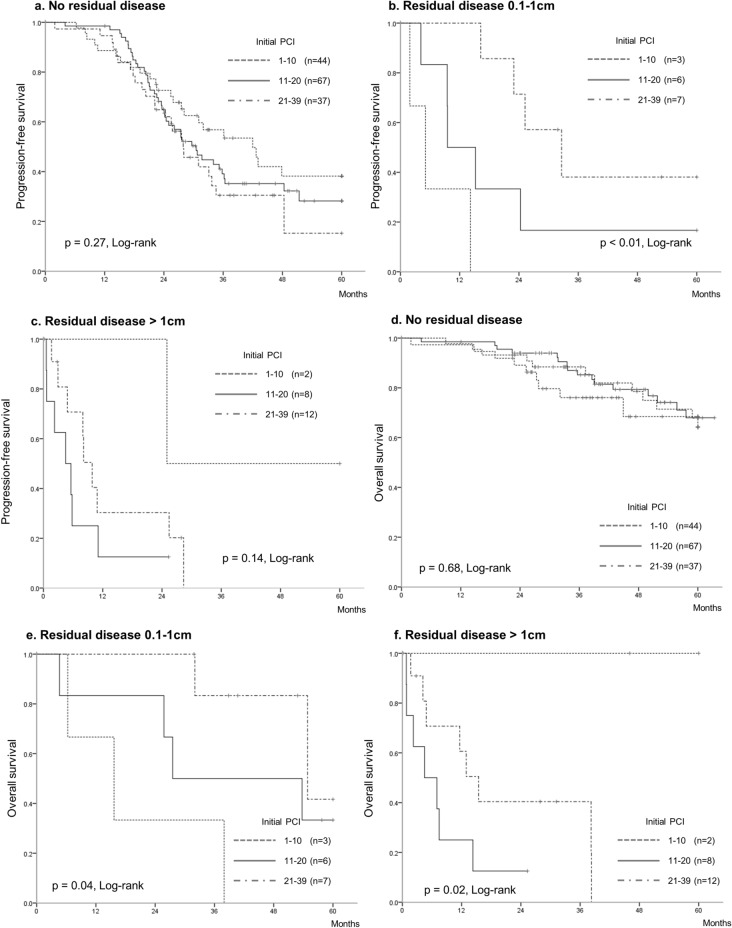
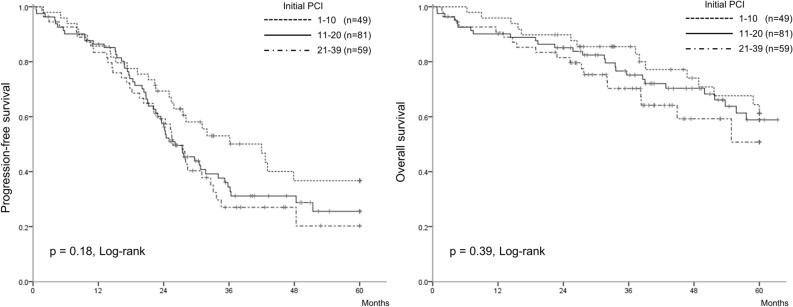
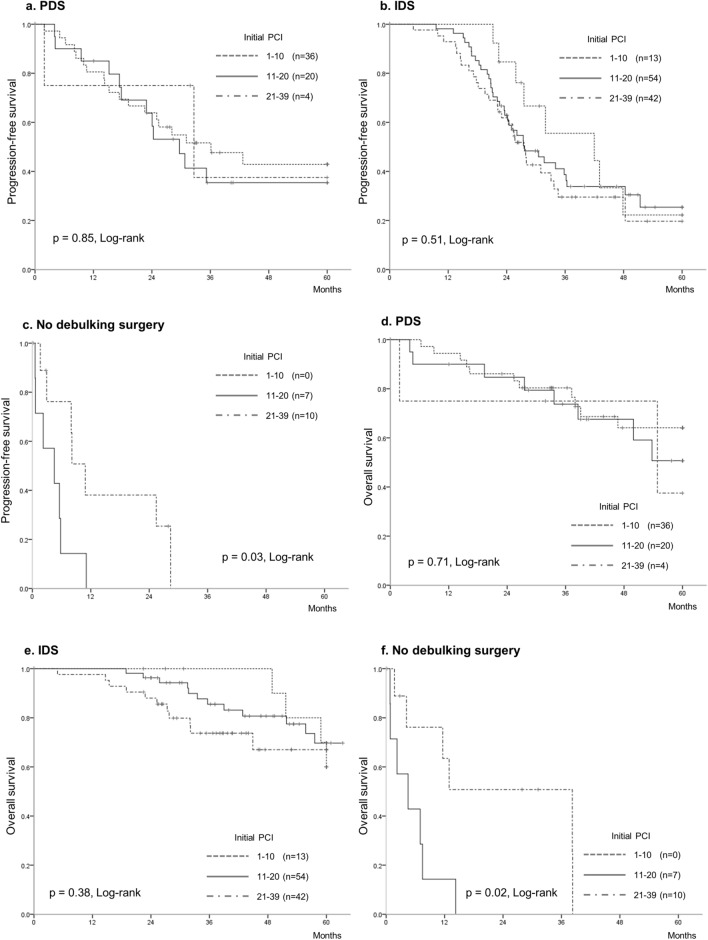
We examined whether the extent of initial peritoneal dissemination affected the prognosis of patients with advanced ovarian, fallopian tube, and peritoneal carcinoma when initially disseminated lesions > 1 cm in diameter were removed, regardless of the timing of aggressive cytoreductive surgery. The extent of peritoneal dissemination was assessed by the peritoneal cancer index (PCI) at initial laparotomy in 186 consecutive patients with stage IIIC/IV. Sixty patients underwent primary debulking surgery and 109 patients underwent neoadjuvant chemotherapy followed by interval debulking surgery. Seventeen patients could not undergo debulking surgery because of disease progression during neoadjuvant chemotherapy. The median initial PCI were 17. Upper abdominal surgery and bowel resection were performed in 149 (80%) and 171 patients (92%), respectively. Residual disease ≤ 1 cm after surgery was achieved in 164 patients (89%). The initial PCI was not significantly associated with progression-free survival (PFS; p = 0.13) and overall survival (OS; p = 0.09). No residual disease and a high-complexity surgery significantly prolonged PFS (p < 0.01 and p = 0.02, respectively) and OS (p < 0.01 and p ≤ 0.01, respectively). The extent of initial peritoneal dissemination did not affect the prognosis when initially disseminated lesions > 1 cm were resected.
我们研究了在初始直径大于 1cm 的播散性病变被切除的情况下,无论积极的细胞减灭术的时机如何,初始腹膜播散的程度是否会影响晚期卵巢、输卵管和腹膜癌患者的预后。在 186 例 IIIC/IV 期连续患者的初次剖腹手术中,通过腹膜癌指数(PCI)评估腹膜播散的程度。60 例患者接受了初次肿瘤细胞减灭术,109 例患者接受了新辅助化疗,然后进行间隔性肿瘤细胞减灭术。17 例患者因新辅助化疗期间疾病进展而无法进行肿瘤细胞减灭术。中位数初始 PCI 为 17。149 例(80%)和 171 例(92%)患者分别进行了上腹部手术和肠切除术。术后 164 例(89%)达到了残余疾病≤1cm。初始 PCI 与无进展生存期(PFS;p=0.13)和总生存期(OS;p=0.09)均无显著相关性。无残留疾病和高复杂度手术显著延长了 PFS(p<0.01 和 p=0.02)和 OS(p<0.01 和 p≤0.01)。当切除初始直径大于 1cm 的播散性病变时,初始腹膜播散的程度并不影响预后。