Department of Intensive Care Medicine, Ghent University Hospital.
Renal Division, Ghent University Hospital.
Ann Am Thorac Soc. 2021 May;18(5):830-837. doi: 10.1513/AnnalsATS.202004-385OC.
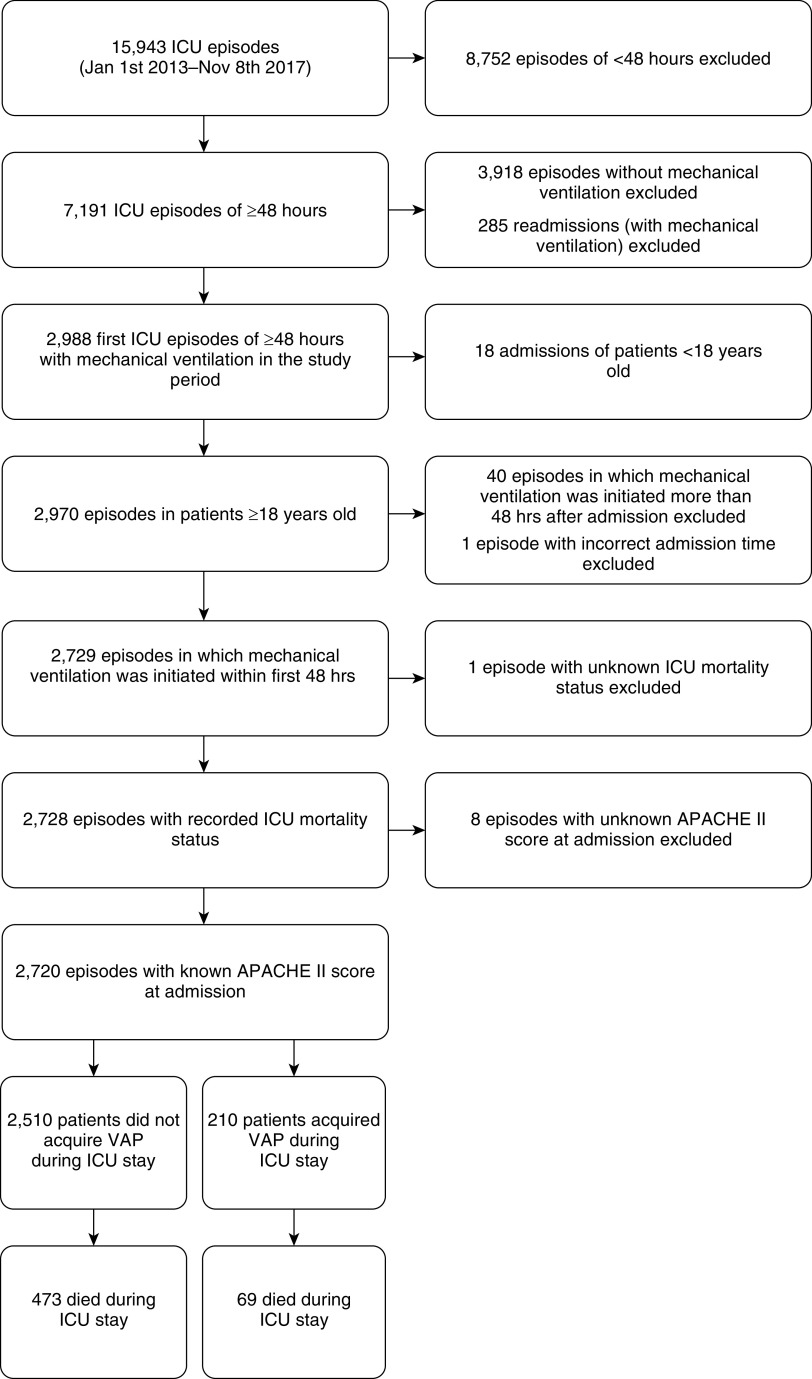
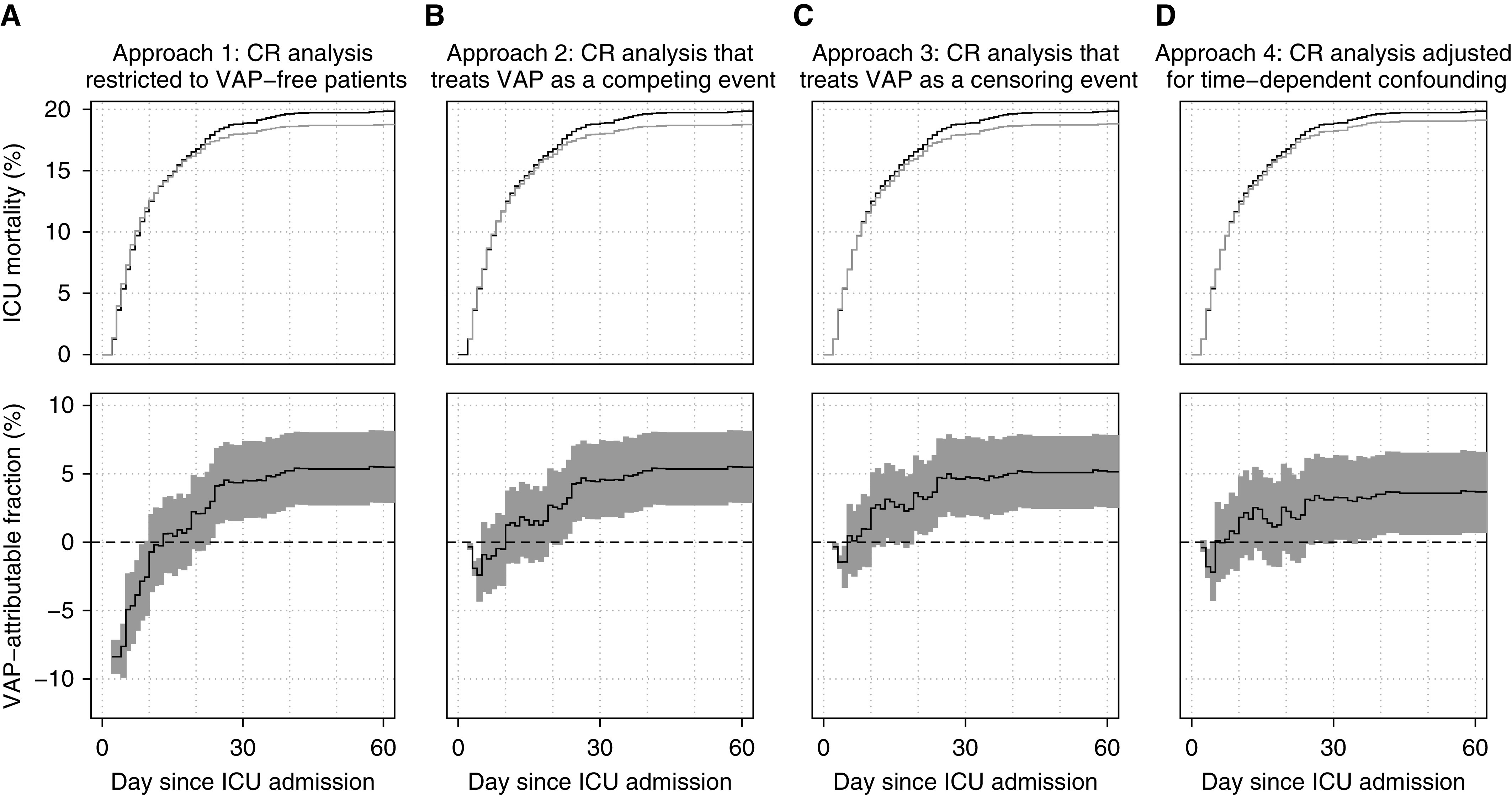
Estimating the impact of ventilator-associated pneumonia (VAP) from routinely collected intensive care unit (ICU) data is methodologically challenging. We aim to replicate earlier findings of limited VAP-attributable ICU mortality in an independent cohort. By refining statistical analyses, we gradually tackle different sources of bias. Records of 2,720 adult patients admitted to Ghent University Hospital ICUs (2013-2017) and receiving mechanical ventilation within 48 hours after admission were extracted from linked Intensive Care Information System and Computer-based Surveillance and Alerting of Nosocomial Infections, Antimicrobial Resistance, and Antibiotic Consumption in the ICU databases. The VAP-attributable fraction of ICU mortality was estimated using a competing risk analysis that is restricted to VAP-free patients (approach 1), accounts for VAP onset by treating it as either a competing (approach 2) or censoring event (approach 3), or additionally adjusts for time-dependent confounding via inverse probability weighting (approach 4). A total of 210 patients (7.7%) acquired VAP. Based on benchmark approach 4, we estimated that (compared with current preventive measures) hypothetical eradication of VAP would lead to a relative ICU mortality reduction of 1.7% (95% confidence interval, -1.3 to 4.6) by Day 10 and of 3.6% (95% confidence interval, 0.7 to 6.5) by Day 60. Approaches 1-3 produced estimates ranging from -0.7% to 2.5% by Day 10 and from 5.2% to 5.5% by Day 60. In line with previous studies using appropriate methodology, we found limited VAP-attributable ICU mortality given current state-of-the-art VAP prevention measures. Our study illustrates that inappropriate accounting of the time dependency of exposure and confounding of its effects may misleadingly suggest protective effects of early-onset VAP and systematically overestimate attributable mortality.
从常规收集的重症监护病房 (ICU) 数据中估计呼吸机相关性肺炎 (VAP) 的影响在方法学上具有挑战性。我们旨在复制早期在独立队列中发现的有限 VAP 可归因于 ICU 死亡率的发现。通过改进统计分析,我们逐渐解决了不同的偏倚来源。从 ICU 信息系统和基于计算机的医院感染、抗菌药物耐药性和 ICU 抗生素使用监测和警报系统中提取了 2013 年至 2017 年期间入住根特大学医院 ICU 的 2720 名成年患者的记录,这些患者在入院后 48 小时内接受了机械通气。使用竞争风险分析估计 ICU 死亡率的 VAP 归因部分,该分析仅限于无 VAP 患者(方法 1),通过将其视为竞争(方法 2)或删失事件(方法 3)来考虑 VAP 发病,或者通过逆概率加权(方法 4)进一步调整时间依赖性混杂。共有 210 名患者(7.7%)发生 VAP。基于基准方法 4,我们估计(与当前预防措施相比)假设消除 VAP 将导致第 10 天 ICU 死亡率相对降低 1.7%(95%置信区间,-1.3 至 4.6),第 60 天降低 3.6%(95%置信区间,0.7 至 6.5)。方法 1-3 在第 10 天产生的估计值范围为-0.7%至 2.5%,在第 60 天产生的估计值范围为 5.2%至 5.5%。与之前使用适当方法学的研究一致,我们发现,考虑到当前最先进的 VAP 预防措施,VAP 可归因于 ICU 死亡率有限。我们的研究表明,不恰当地考虑暴露的时间依赖性及其影响的混杂可能会错误地暗示早期发病的 VAP 具有保护作用,并系统地高估归因于死亡率。