Department of Medicine and Division of Hematology/Oncology, University of Pittsburgh, School of Medicine, Pittsburgh, PA 15213, USA.
Department of Medicine and Division of Hematology/Oncology, University of Pittsburgh, School of Medicine, Pittsburgh, PA 15213, USA; Department of Immunology, University of Pittsburgh, School of Medicine, Pittsburgh, PA 15213, USA.
Semin Immunol. 2020 Jun;49:101436. doi: 10.1016/j.smim.2020.101436. Epub 2020 Dec 4.
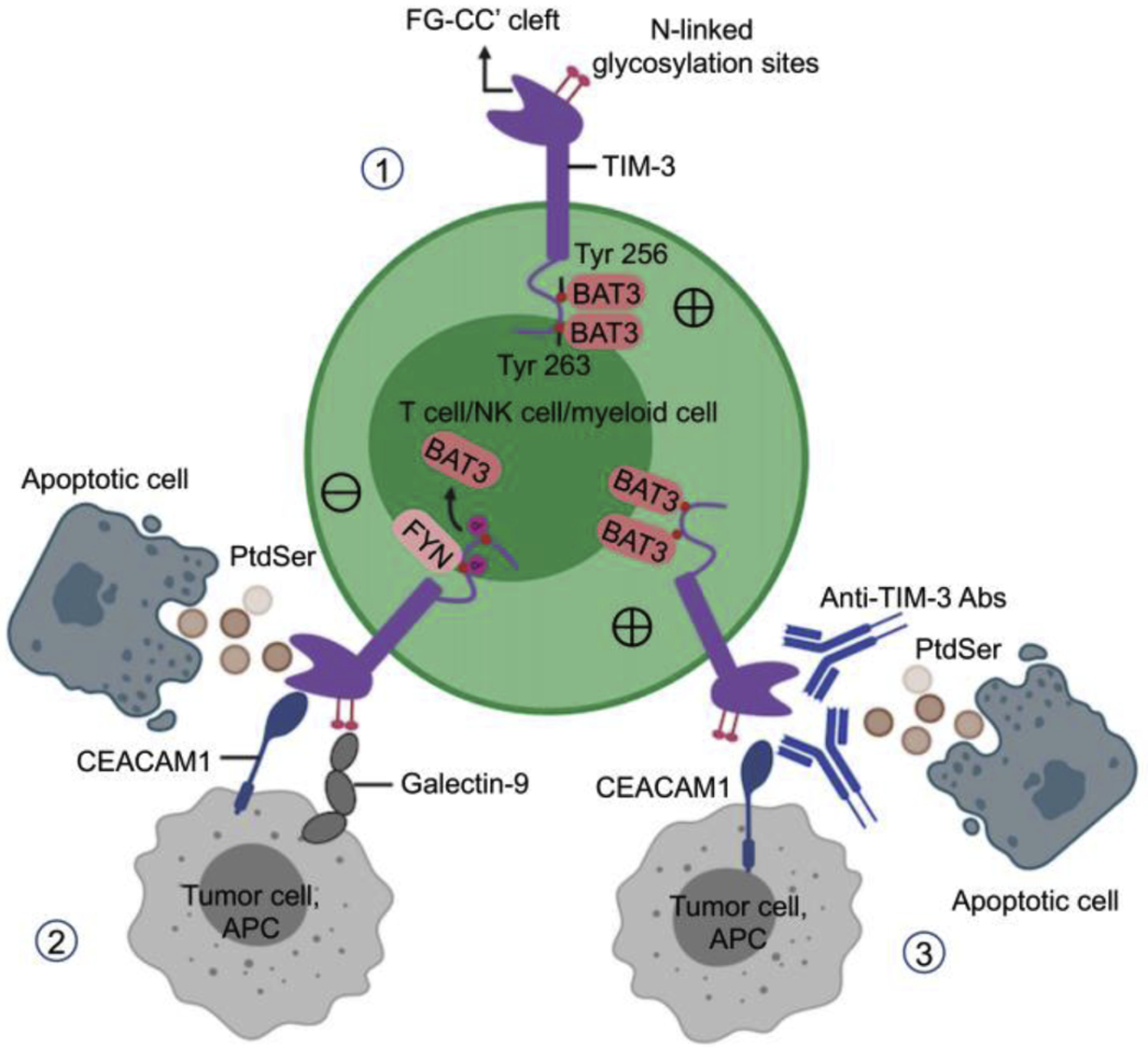
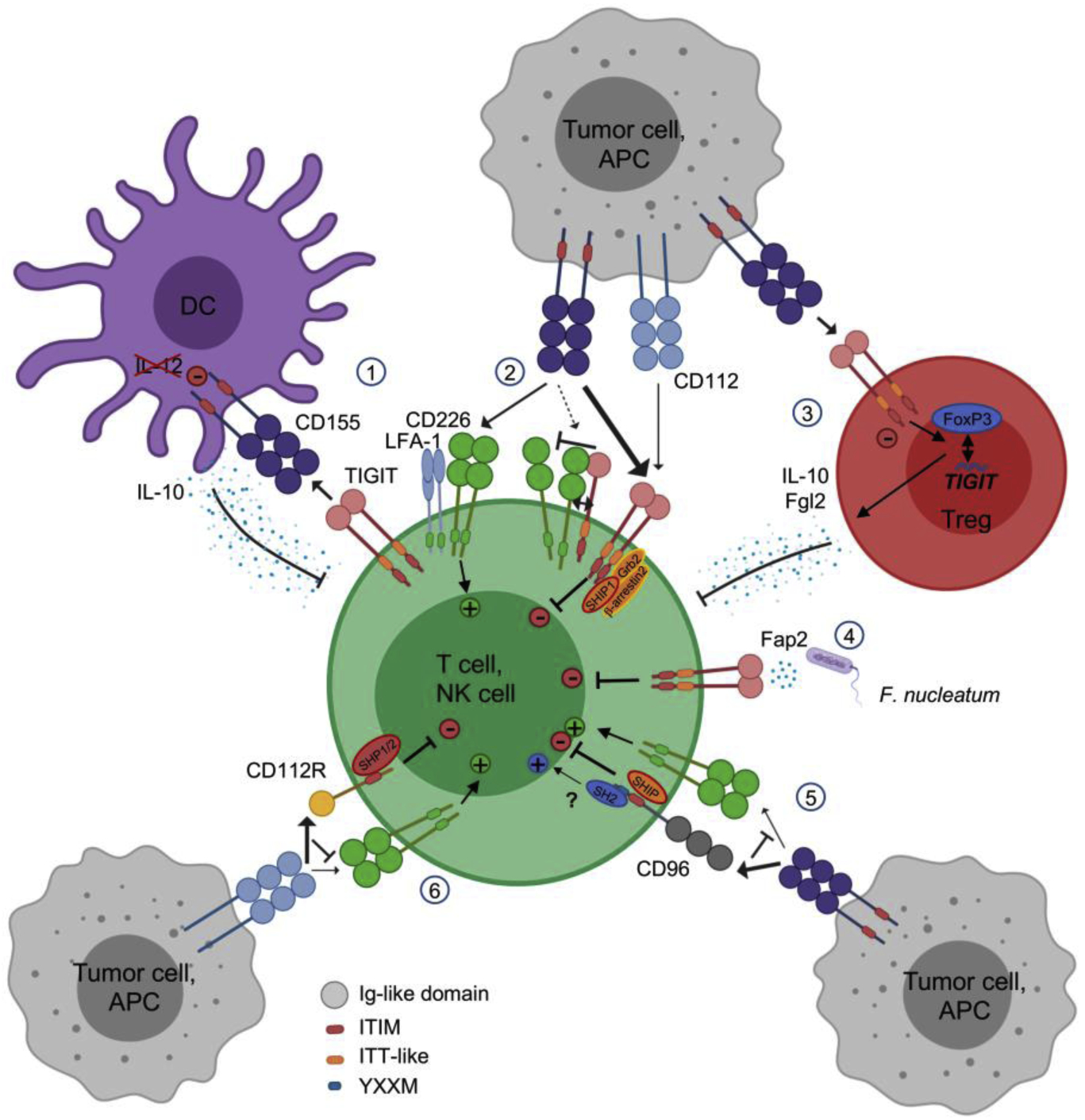
T cells play a critical role in promoting tumor regression in both experimental models and humans. Yet, T cells that are chronically exposed to tumor antigen during cancer progression can become dysfunctional/exhausted and fail to induce tumor destruction. Such tumor-induced T cell dysfunction may occur via multiple mechanisms. In particular, immune checkpoint inhibitory receptors that are upregulated by tumor-infiltrating lymphocytes in many cancers limit T cell survival and function. Overcoming this inhibitory receptor-mediated T cell dysfunction has been a central focus of recent developments in cancer immunotherapy. Immunotherapies targeting inhibitory receptor pathways such as programmed cell death 1 (PD-1)/programmed death ligand 1 and cytotoxic T lymphocyte-associated antigen 4 (CTLA-4), alone or in combination, confer significant clinical benefits in multiple tumor types. However, many patients with cancer do not respond to immune checkpoint blockade, and dual PD-1/CTLA-4 blockade may cause serious adverse events, which limits its indications. Targeting novel non-redundant inhibitory receptor pathways contributing to tumor-induced T cell dysfunction in the tumor microenvironment may prove efficacious and non-toxic. This review presents preclinical and clinical findings supporting the roles of two key pathways-T-cell immunoglobulin and mucin-domain containing-3 (TIM-3) and T cell immunoreceptor with Ig and ITIM domain (TIGIT)/CD226/CD96/CD112R-in cancer immunotherapy.
T 细胞在促进实验模型和人类肿瘤消退中发挥着关键作用。然而,在癌症进展过程中,长期暴露于肿瘤抗原的 T 细胞会变得功能失调/衰竭,无法诱导肿瘤破坏。这种肿瘤诱导的 T 细胞功能障碍可能通过多种机制发生。特别是,在许多癌症中,浸润肿瘤的淋巴细胞上调的免疫检查点抑制受体限制了 T 细胞的存活和功能。克服这种抑制性受体介导的 T 细胞功能障碍一直是癌症免疫治疗最新进展的核心关注点。针对抑制性受体途径的免疫疗法,如程序性细胞死亡 1 (PD-1)/程序性死亡配体 1 和细胞毒性 T 淋巴细胞相关抗原 4 (CTLA-4),单独或联合使用,在多种肿瘤类型中都能带来显著的临床获益。然而,许多癌症患者对免疫检查点阻断无反应,而双重 PD-1/CTLA-4 阻断可能会导致严重的不良反应,从而限制了其适应证。针对肿瘤微环境中导致肿瘤诱导的 T 细胞功能障碍的新型非冗余抑制性受体途径可能具有疗效和无毒的优势。本文综述了支持 T 细胞免疫球蛋白和粘蛋白结构域包含 3 (TIM-3)和 T 细胞免疫受体 Ig 和 ITIM 结构域 (TIGIT)/CD226/CD96/CD112R 这两条关键途径在癌症免疫治疗中的作用的临床前和临床研究结果。