Division of Regenerative Dentistry and Periodontology, University Clinics of Dental Medicine (CUMD), University of Geneva, Geneva, Switzerland.
Department of Periodontology, Faculty of Odontology, University of Malmö, Sweden.
J Clin Periodontol. 2021 Mar;48(3):410-430. doi: 10.1111/jcpe.13409. Epub 2021 Jan 21.
Systematic reviews have established the short-term improvements of periodontal regenerative/reconstructive procedures compared to conventional surgical treatment in intrabony defects. However, a hierarchy of periodontal regenerative/reconstructive procedures regarding the medium- to long-term results of treatment does not exist.
To systematically assess the literature to answer the focused question "In periodontitis patients with intrabony defects, what are the medium- and long-term benefits of periodontal regenerative/reconstructive procedures compared with open flap debridement (OFD), in terms of clinical and/or radiographic outcome parameters and tooth retention?".
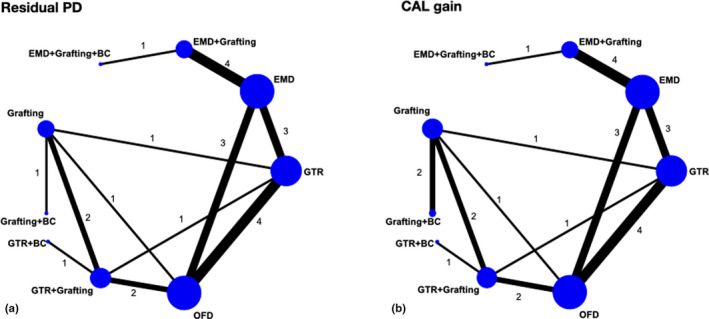
MATERIAL & METHODS: Randomized controlled clinical trials (RCTs), reporting on clinical and/or radiographic outcome parameters of periodontal regenerative/reconstructive procedures ≥3 years post-operatively, were systematically assessed. Clinical [residual probing pocket depth (PD) and clinical attachment level (CAL) gain, tooth loss] and radiographic [residual defect depth (RDD), bone gain (RBL)] outcome parameters were assessed. Descriptive statistics were calculated, and Bayesian random-effects network meta-analyses (NMA) were performed where possible.
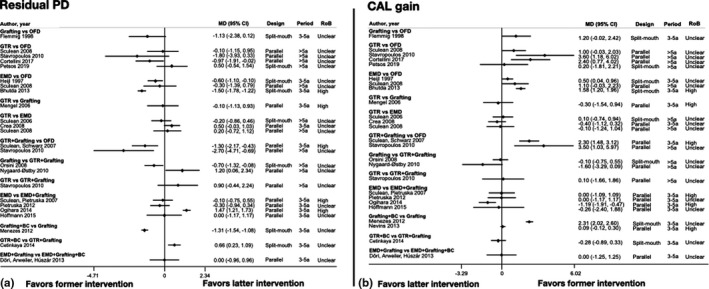
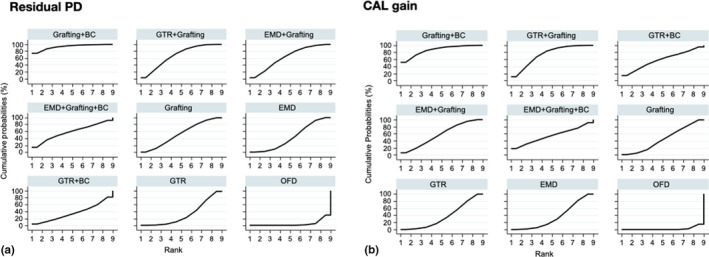
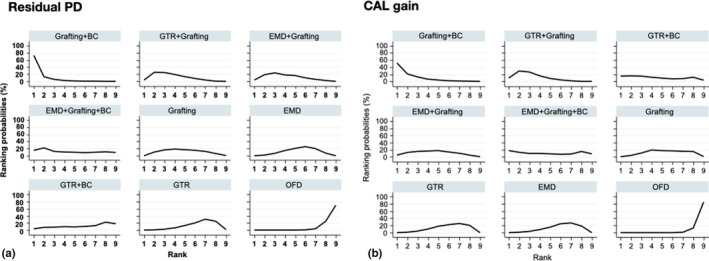
Thirty RCTs, presenting data 3 to 20 years after treatment with grafting, GTR, EMD, as monotherapies, combinations thereof, and/or adjunctive use of blood-derived growth factor constructs or with OFD only, were included. NMA based on 21 RCTs showed that OFD was clearly the least efficacious treatment; regenerative/reconstructive treatments resulted in significantly shallower residual PD in 4 out 8 comparisons [range of mean differences (MD): -2.37 to -0.60 mm] and larger CAL gain in 6 out 8 comparisons (range of MD: 1.26 to 2.66 mm), and combination approaches appeared as the most efficacious. Tooth loss after regenerative/reconstructive treatment was less frequent (0.4%) compared to OFD (2.8%), but the evidence was sparse. There were only sparse radiographic data not allowing any relevant comparisons.
Periodontal regenerative/reconstructive therapy in intrabony defects results, in general, in shallower residual PD and larger CAL gain compared with OFD, translating in high rates of tooth survival, on a medium (3-5 years) to long-term basis (5-20 years). Combination approaches appear, in general, more efficacious compared to monotherapy in terms of shallower residual PD and larger CAL gain. A clear hierarchy could, however, not be established due to limited evidence.
系统评价已经证实,与传统手术治疗相比,牙周再生/重建程序在骨内缺损方面具有短期改善效果。然而,针对牙周再生/重建程序在中-长期治疗效果方面,并不存在一种分层体系。
系统评估文献,以回答以下具体问题:“在患有骨内缺损的牙周炎患者中,与翻瓣清创术(OFD)相比,牙周再生/重建程序在中-长期内,从临床和/或影像学结果参数以及保留牙齿的角度来看,具有哪些优势?”
系统性评估了随机对照临床试验(RCT),这些 RCT 报告了牙周再生/重建程序在术后至少 3 年的临床和/或影像学结果参数。评估了临床(剩余探诊深度(PD)和临床附着水平(CAL)的获得、牙齿缺失)和影像学(剩余缺损深度(RDD)、骨获得(RBL))的结果参数。计算了描述性统计数据,并在可能的情况下进行了贝叶斯随机效应网络荟萃分析(NMA)。
纳入了 30 项 RCT,这些 RCT 在单独使用移植物、GTR、EMD 或联合使用血液衍生生长因子构建体或仅进行 OFD 治疗后 3 至 20 年报告了数据。基于 21 项 RCT 的 NMA 结果显示,OFD 是最无效的治疗方法;再生/重建治疗在 8 项比较中有 4 项(平均差值(MD)范围:-2.37 至-0.60mm)和 6 项比较中(MD 范围:1.26 至 2.66mm)具有明显更浅的剩余 PD,且联合治疗方法的效果似乎最佳。与 OFD(2.8%)相比,再生/重建治疗后的牙齿缺失频率较低(0.4%),但证据稀疏。仅有少量的放射影像学数据,不允许进行任何相关比较。
与 OFD 相比,骨内缺损的牙周再生/重建治疗通常会导致更浅的剩余 PD 和更大的 CAL 获得,从而在中短期(3-5 年)至长期(5-20 年)内保持较高的牙齿存活率。与单药治疗相比,联合治疗方法在剩余 PD 变浅和 CAL 获得更大方面通常更有效。然而,由于证据有限,因此无法确定明确的分层体系。