Department of Radiology, Shengjing Hospital of China Medical University, Shenyang, China.
Department of Cardiology, Shengjing Hospital of China Medical University, Shenyang, China.
Korean J Radiol. 2021 Apr;22(4):535-546. doi: 10.3348/kjr.2019.0969. Epub 2020 Nov 30.
To evaluate the feasibility of texture analysis on non-contrast-enhanced T1 maps of cardiac magnetic resonance (CMR) imaging for the diagnosis of myocardial injury in acute myocardial infarction (MI).
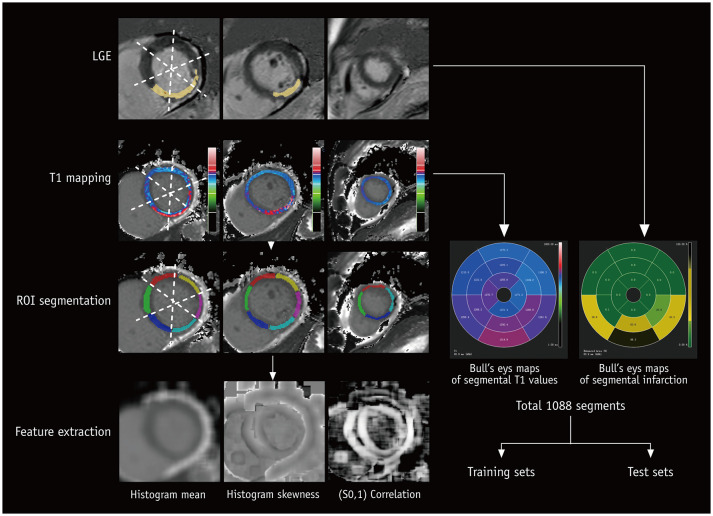
This study included 68 patients (57 males and 11 females; mean age, 55.7 ± 10.5 years) with acute ST-segment-elevation MI who had undergone 3T CMR after a percutaneous coronary intervention. Forty patients of them also underwent a 6-month follow-up CMR. The CMR protocol included T2-weighted imaging, T1 mapping, rest first-pass perfusion, and late gadolinium enhancement. Radiomics features were extracted from the T1 maps using open-source software. Radiomics signatures were constructed with the selected strongest features to evaluate the myocardial injury severity and predict the recovery of left ventricular (LV) longitudinal systolic myocardial contractility.
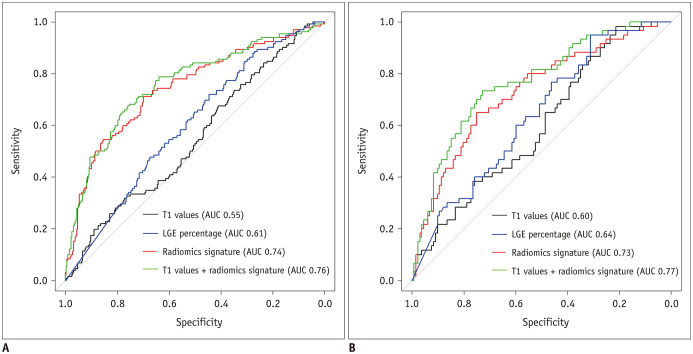
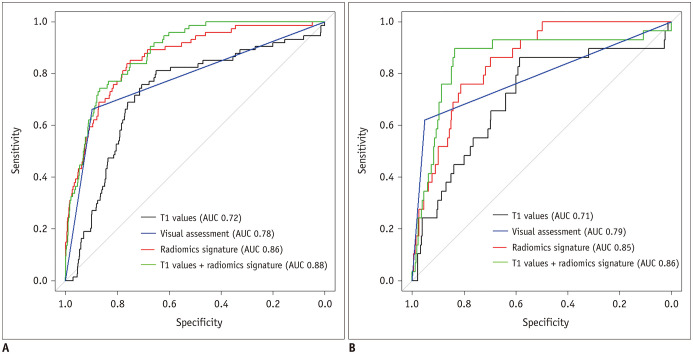
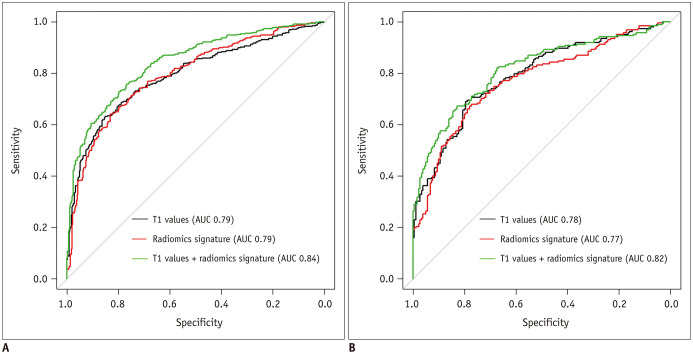
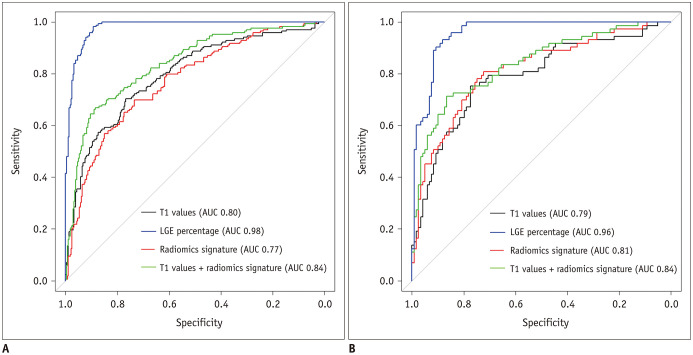
A total of 1088 segments of the acute CMR images were analyzed; 103 (9.5%) segments showed microvascular obstruction (MVO), and 557 (51.2%) segments showed MI. A total of 640 segments were included in the 6-month follow-up analysis, of which 160 (25.0%) segments showed favorable recovery of LV longitudinal systolic myocardial contractility. Combined radiomics signature and T1 values resulted in a higher diagnostic performance for MVO compared to T1 values alone (area under the curve [AUC] in the training set; 0.88, 0.72, = 0.031: AUC in the test set; 0.86, 0.71, p002). Combined radiomics signature and T1 values also provided a higher predictive value for LV longitudinal systolic myocardial contractility recovery compared to T1 values (AUC in the training set; 0.76, 0.55, < 0.001: AUC in the test set; 0.77, 0.60, < 0.001).
The combination of radiomics of non-contrast-enhanced T1 mapping and T1 values could provide higher diagnostic accuracy for MVO. Radiomics also provides incremental value in the prediction of LV longitudinal systolic myocardial contractility at six months.
评估心脏磁共振(CMR)成像平扫 T1 图纹理分析用于诊断急性心肌梗死(MI)心肌损伤的可行性。
本研究纳入了 68 例(男 57 例,女 11 例;平均年龄 55.7±10.5 岁)接受经皮冠状动脉介入治疗后行 3T CMR 的急性 ST 段抬高型 MI 患者。其中 40 例患者进行了 6 个月的 CMR 随访。CMR 方案包括 T2 加权成像、T1 映射、静息首过灌注和晚期钆增强。使用开源软件从 T1 图谱中提取放射组学特征。使用选定的最强特征构建放射组学特征,以评估心肌损伤严重程度并预测左心室(LV)纵向收缩心肌收缩力的恢复情况。
共分析了 1088 个急性 CMR 图像节段;其中 103 个(9.5%)节段显示微血管阻塞(MVO),557 个(51.2%)节段显示 MI。共有 640 个节段纳入 6 个月的随访分析,其中 160 个(25.0%)节段显示 LV 纵向收缩心肌收缩力的恢复良好。与 T1 值相比,联合放射组学特征和 T1 值对 MVO 的诊断性能更高(训练集的曲线下面积[AUC];0.88、0.72,=0.031;测试集的 AUC;0.86、0.71,p002)。与 T1 值相比,联合放射组学特征和 T1 值对 LV 纵向收缩心肌收缩力恢复的预测价值也更高(训练集的 AUC;0.76、0.55,<0.001;测试集的 AUC;0.77、0.60,<0.001)。
联合非对比增强 T1 映射的放射组学和 T1 值可以提高对 MVO 的诊断准确性。放射组学还可以提高对 6 个月时 LV 纵向收缩心肌收缩力的预测价值。