Division of Gastroenterology and Hepatology, Department of Internal Medicine III, Medical University of Vienna, Währinger Gürtel 18-20, 1090, Vienna, Austria.
Vienna Hepatic Hemodynamic Laboratory, Medical University of Vienna, Vienna, Austria.
Hepatol Int. 2020 Dec;14(6):1093-1103. doi: 10.1007/s12072-020-10112-3. Epub 2020 Dec 8.
The liver plays a key role in the storage, metabolism and homeostasis of fat-soluble vitamins. We investigated the relation of Vitamin(Vit)A/D/E serum levels with severity of liver disease and portal hypertension (PHT).
VitA/D/E serum levels were assessed in 234 patients with advanced chronic liver disease (ACLD, i.e. hepatic venous pressure gradient [HVPG] ≥ 6 mmHg). Patients with hepatocellular carcinoma, pre-/post-hepatic PHT, TIPS or liver transplantation were excluded.
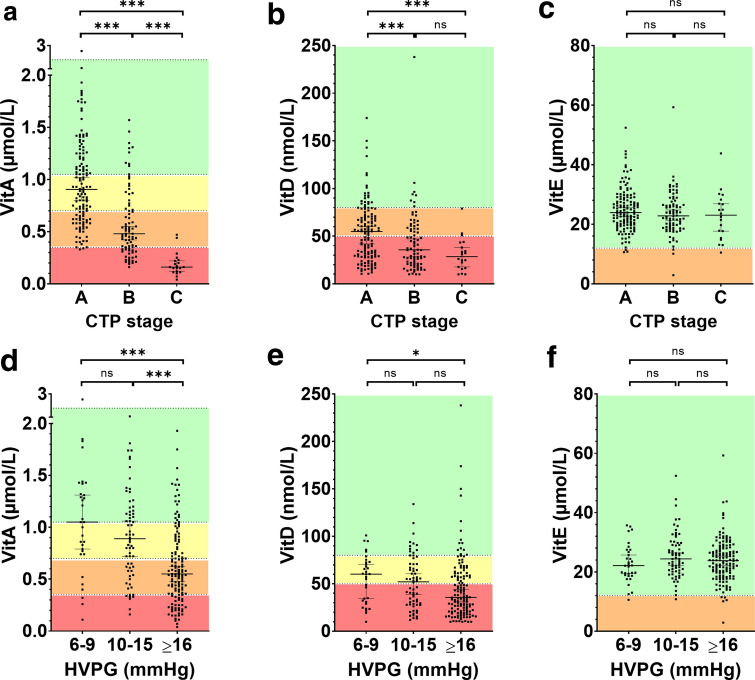
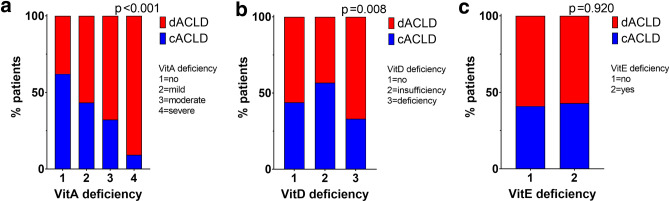
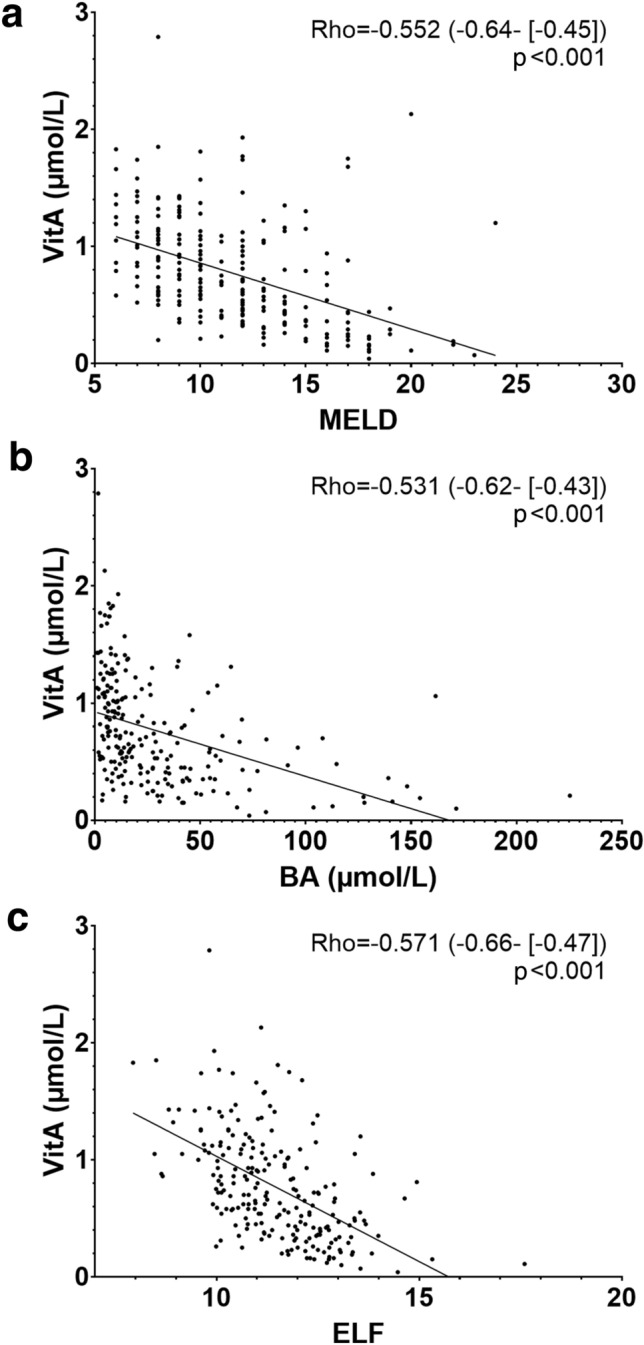
Most patients were male (n = 153; 65%) with a median age of 57.6 (49.7-64.5) years. Thirty-two (14%) patients had HVPG 6-9 mmHg, 66 (28%) 10-15 mmHg, and 136 (58%) ≥ 16 mmHg, respectively. VitD deficiency (25-OH-vitamin-D <50 nmol/L) was found in 133 (57%) with higher prevalence in Child-Turcotte-Pugh (CTP)-C: 85% vs. B: 66% vs. A: 47% (p < 0.001). VitD levels displayed significant but weak correlations with hepatic dysfunction and PHT. VitE levels were normal in 227 (97%) patients and displayed no relevant association with hepatic dysfunction or PHT. Only 63 (27%) patients had normal (>1.05 µmol/L) VitA levels, while 58 (25%) had mild (0.70-1.04 µmol/L), 71 (30%) moderate (0.35-0.69 µmol/L), and 42(18%) severe(<0.35 µmol/L) VitA deficiency. VitA correlated with HVPG (Rho = -0.409), CTP score (Rho = -0.646), and serum bile acid levels (Rho = -0.531; all p < 0.001). The prevalence of decompensated ACLD (dACLD) continuously increased with severity of VitA deficiency (no: 40% vs. mild: 51% vs. moderate: 67% vs. severe: 91% had dACLD; p < 0.001). CTP score (per point; OR 2.46; 95%CI 1.80-3.37; p <0.001), age (per year; OR 0.95; 95%CI 0.92-0.98; p = 0.001) and elevated bile acid levels(>10 µmol/L; OR 3.62; 95%CI 1.61-8.14; p = 0.002) were independently associated with VitA deficiency.
VitA and VitD but not VitE deficiencies are highly prevalent in ACLD. VitA deficiency strongly correlates with hepatic dysfunction, PHT and bile acid levels and is associated with decompensated ACLD.
NCT03267615.
肝脏在脂溶性维生素的储存、代谢和内稳态中起着关键作用。我们研究了维生素 A/D/E 血清水平与肝脏疾病严重程度和门静脉高压(PHT)的关系。
我们评估了 234 例晚期慢性肝病(ACLD,即肝静脉压力梯度[HVPG]≥6mmHg)患者的维生素 A/D/E 血清水平。排除了肝细胞癌、前/后 PHT、TIPS 或肝移植患者。
大多数患者为男性(n=153;65%),中位年龄为 57.6(49.7-64.5)岁。32 例(14%)患者 HVPG 为 6-9mmHg,66 例(28%)为 10-15mmHg,136 例(58%)≥16mmHg。25-羟维生素 D(25-OH-vitamin-D<50nmol/L)缺乏症在 133 例(57%)患者中发现,Child-Turcotte-Pugh(CTP)-C 患者中更为常见:85%比 B 组:66%比 A 组:47%(p<0.001)。维生素 D 水平与肝功能障碍和 PHT 呈显著但弱相关。227 例(97%)患者维生素 E 水平正常,与肝功能障碍或 PHT 无相关。仅有 63 例(27%)患者维生素 A 水平正常(>1.05μmol/L),而 58 例(25%)患者维生素 A 轻度缺乏(0.70-1.04μmol/L),71 例(30%)患者维生素 A 中度缺乏(0.35-0.69μmol/L),42 例(18%)患者维生素 A 严重缺乏(<0.35μmol/L)。维生素 A 与 HVPG(Rho=-0.409)、CTP 评分(Rho=-0.646)和血清胆汁酸水平(Rho=-0.531;均 p<0.001)呈负相关。随着维生素 A 缺乏程度的加重(无:40% vs. 轻度:51% vs. 中度:67% vs. 严重:91%患有失代偿性 ACLD;p<0.001),失代偿性 ACLD 的发生率持续增加。CTP 评分(每分;OR 2.46;95%CI 1.80-3.37;p<0.001)、年龄(每年;OR 0.95;95%CI 0.92-0.98;p=0.001)和升高的胆汁酸水平(>10μmol/L;OR 3.62;95%CI 1.61-8.14;p=0.002)与维生素 A 缺乏独立相关。
维生素 A 和维生素 D 但不是维生素 E 缺乏症在 ACLD 中非常常见。维生素 A 缺乏与肝功能障碍、PHT 和胆汁酸水平密切相关,并与失代偿性 ACLD 相关。
NCT03267615。