Kobayashi Tatsuya, Miyazaki Makoto, Sasaki Nobuyoshi, Yamamuro Shun, Uchida Eita, Kawauchi Daisuke, Takahashi Masamichi, Otsuka Yohei, Kumagai Kosuke, Takeuchi Satoru, Toyooka Terushige, Otani Naoki, Wada Kojiro, Narita Yoshitaka, Yamaguchi Hideki, Muragaki Yoshihiro, Kawamata Takakazu, Mori Kentaro, Ichimura Koichi, Tomiyama Arata
Division of Brain Tumor Translational Research, National Cancer Center Research Institute, 5-1-1 Tsukiji, Chuo-ku, Tokyo 104-0045, Japan.
Department of Neurosurgery, National Defense Medical College, 3-2 Namiki, Tokorozawa, Saitama 359-8513, Japan.
Cancers (Basel). 2020 Dec 4;12(12):3641. doi: 10.3390/cancers12123641.
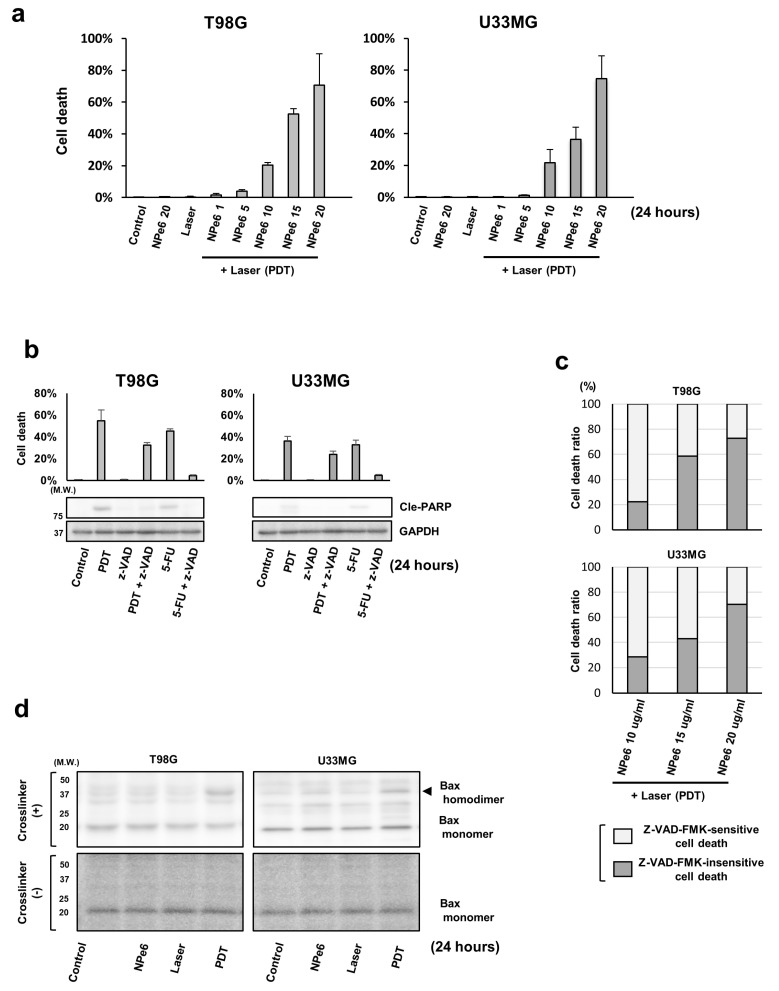
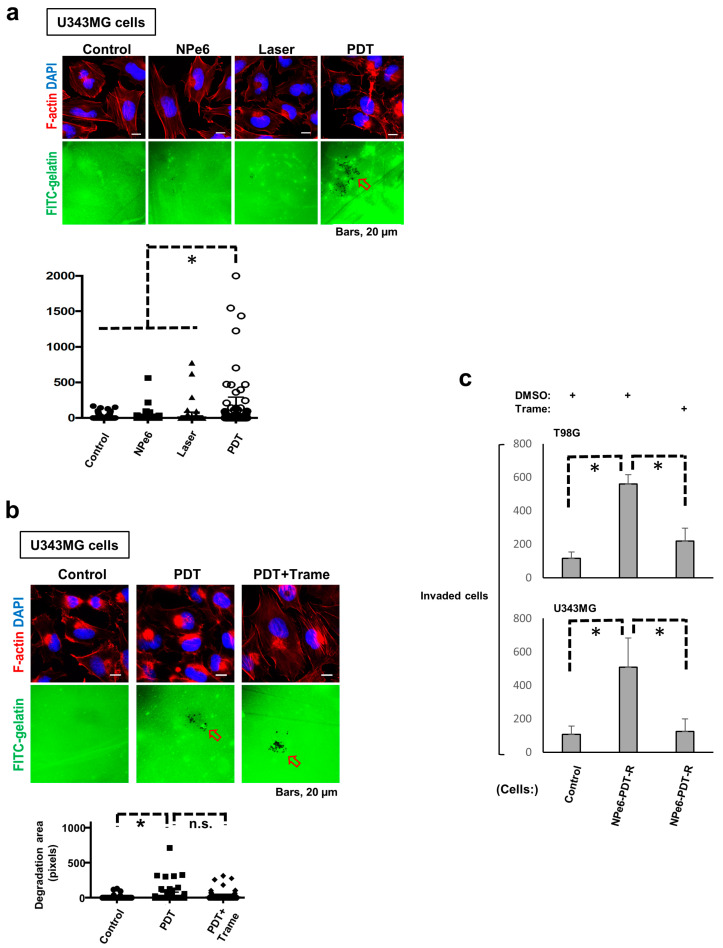
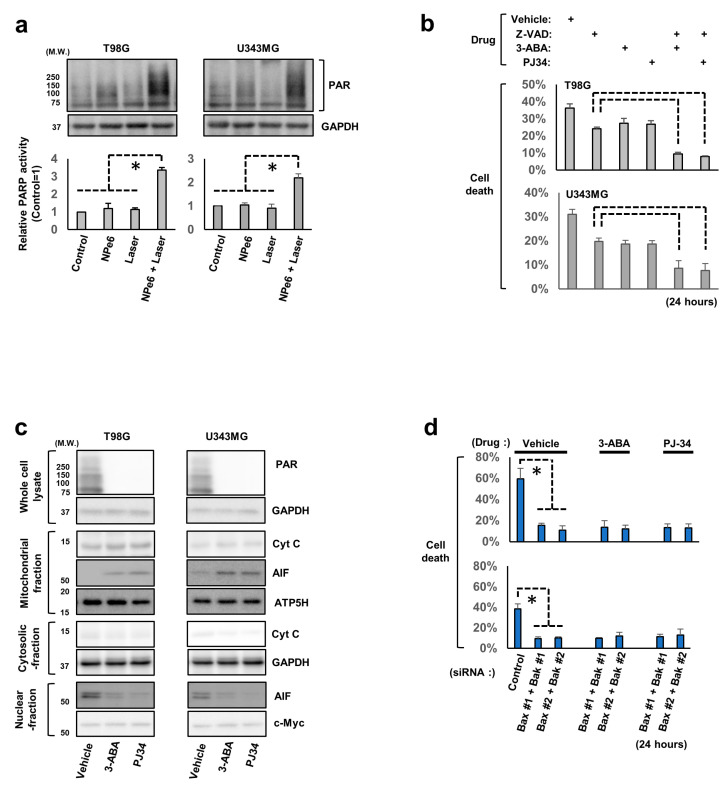
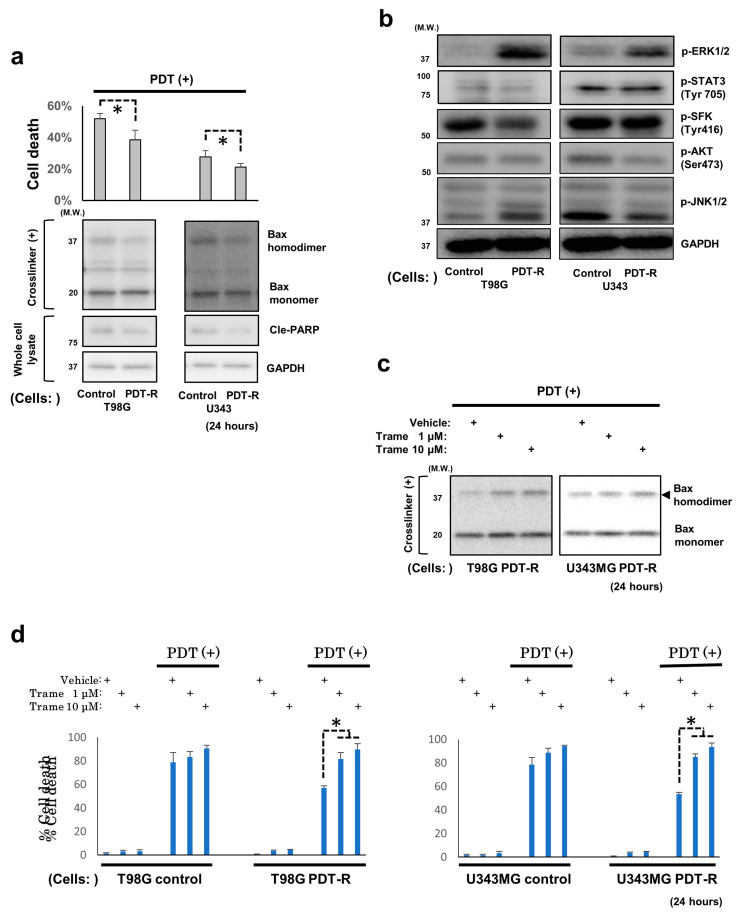
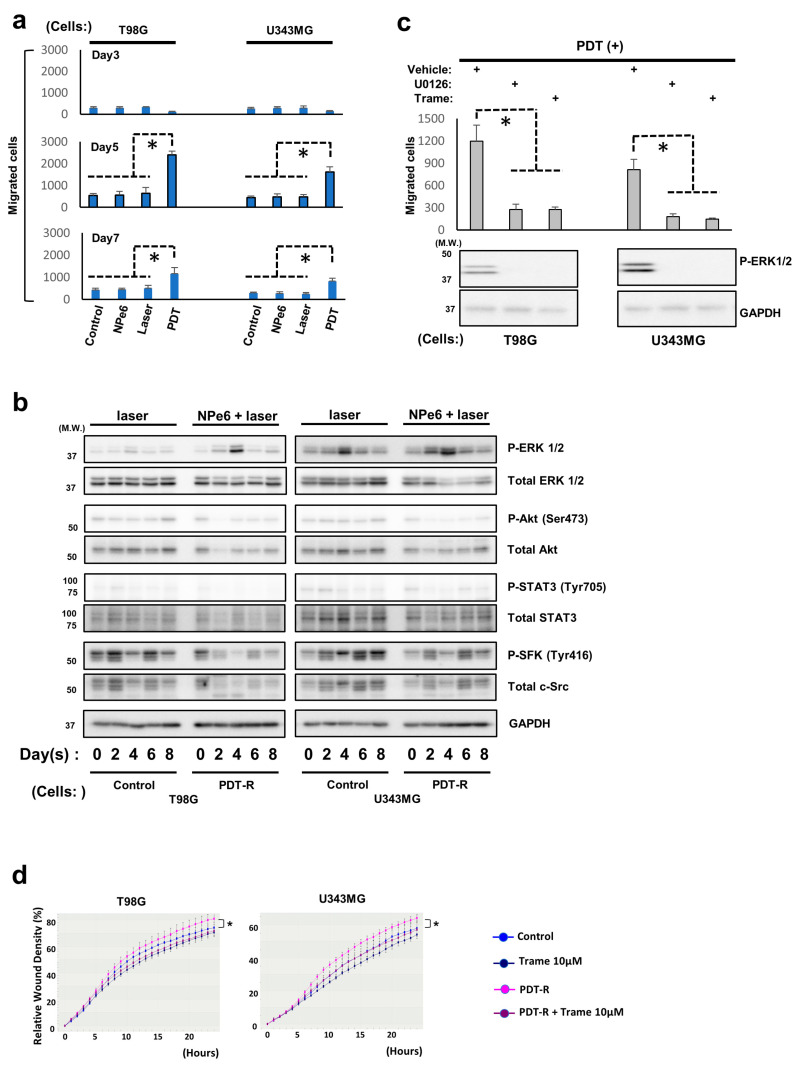
To manage refractory and invasive glioblastomas (GBM)s, photodynamic therapy (PDT) using talaporfin sodium (NPe6) (NPe6-PDT) was recently approved in clinical practice. However, the molecular machineries regulating resistance against NPe6-PDT in GBMs and mechanisms underlying the changes in GBM phenotypes following NPe6-PDT remain unknown. Herein, we established an in vitro NPe6-mediated PDT model using human GBM cell lines. NPe6-PDT induced GBM cell death in a NPe6 dose-dependent manner. However, this NPe6-PDT-induced GBM cell death was not completely blocked by the pan-caspase inhibitor, suggesting NPe6-PDT induces both caspase-dependent and -independent cell death. Moreover, treatment with poly (ADP-ribose) polymerase inhibitor blocked NPe6-PDT-triggered caspase-independent GBM cell death. Next, it was also revealed resistance to re-NPe6-PDT of GBM cells and GBM stem cells survived following NPe6-PDT (NPe6-PDT-R cells), as well as migration and invasion of NPe6-PDT-R cells were enhanced. Immunoblotting of NPe6-PDT-R cells to assess the behavior of the proteins that are known to be stress-induced revealed that only ERK1/2 activation exhibited the same trend as migration. Importantly, treatment with the MEK1/2 inhibitor trametinib reversed resistance against re-NPe6-PDT and suppressed the enhanced migration and invasion of NPe6-PDT-R cells. Overall, enhanced ERK1/2 activation is suggested as a key regulator of elevated malignant phenotypes of GBM cells surviving NPe6-PDT and is therefore considered as a potential therapeutic target against GBM.
为了治疗难治性和侵袭性胶质母细胞瘤(GBM),最近光动力疗法(PDT)使用替拉泊芬钠(NPe6)(NPe6-PDT)已被批准用于临床实践。然而,调节GBM对NPe6-PDT耐药性的分子机制以及NPe6-PDT后GBM表型变化的潜在机制仍不清楚。在此,我们使用人GBM细胞系建立了体外NPe6介导的PDT模型。NPe6-PDT以NPe6剂量依赖性方式诱导GBM细胞死亡。然而,这种NPe6-PDT诱导的GBM细胞死亡并未被泛半胱天冬酶抑制剂完全阻断,这表明NPe6-PDT诱导了半胱天冬酶依赖性和非依赖性细胞死亡。此外,聚(ADP-核糖)聚合酶抑制剂处理可阻断NPe6-PDT触发的半胱天冬酶非依赖性GBM细胞死亡。接下来,还发现GBM细胞和GBM干细胞在NPe6-PDT后存活下来(NPe6-PDT-R细胞)对再NPe6-PDT具有抗性,并且NPe6-PDT-R细胞的迁移和侵袭增强。对NPe6-PDT-R细胞进行免疫印迹以评估已知受应激诱导的蛋白质的行为,结果显示只有ERK1/2激活与迁移表现出相同的趋势。重要的是,用MEK1/2抑制剂曲美替尼治疗可逆转对再NPe6-PDT的抗性,并抑制NPe6-PDT-R细胞增强的迁移和侵袭。总体而言,ERK1/2激活增强被认为是存活于NPe6-PDT后的GBM细胞恶性表型升高的关键调节因子,因此被视为针对GBM的潜在治疗靶点。