Griffin Edward, Hyde Chris, Long Linda, Varley-Campbell Jo, Coelho Helen, Robinson Sophie, Snowsill Tristan
Peninsula Technology Assessment Group (PenTAG), College of Medicine and Health, University of Exeter, St Luke's campus, Heavitree Road, Exeter, EX1 2LU, UK.
Exeter Test Group, College of Medicine and Health, University of Exeter, St Luke's campus, Heavitree Road, Exeter, EX1 2LU, UK.
Diagn Progn Res. 2020 Dec 2;4(1):20. doi: 10.1186/s41512-020-00087-y.
A systematic review of economic evaluations for lung cancer identified no economic models of the UK setting based on disease natural history. We first sought to develop a new model of natural history for population screening, then sought to explore the cost-effectiveness of multiple alternative potential programmes.
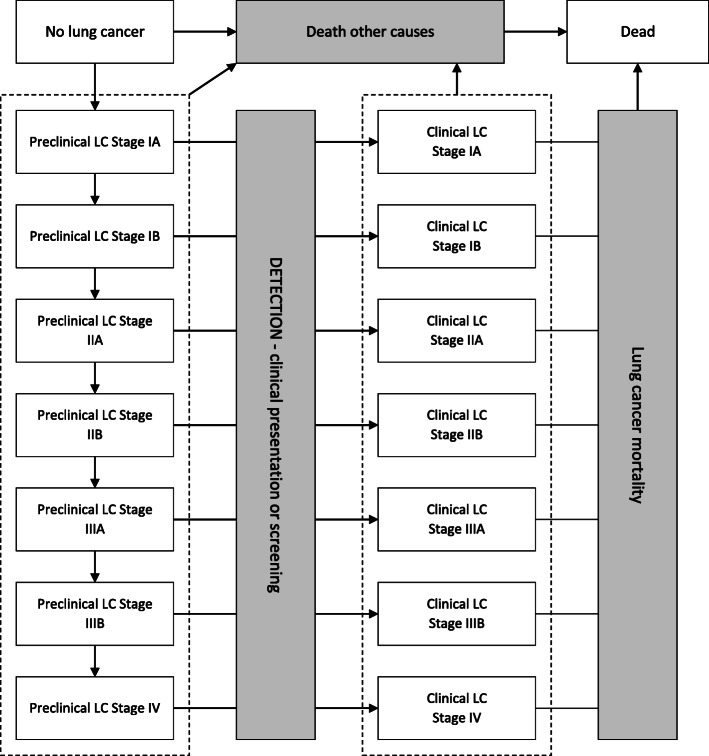
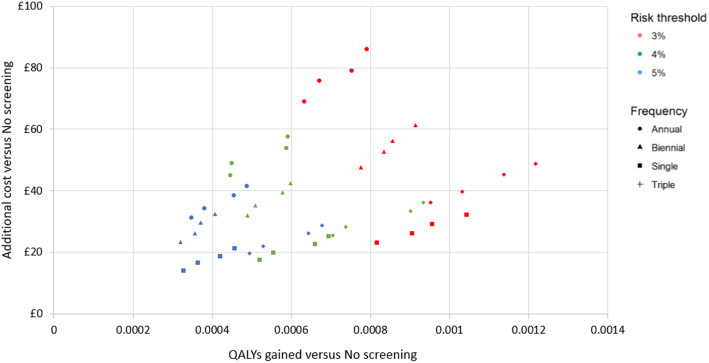
An individual patient model (ENaBL) was constructed in MS Excel® and calibrated against data from the US National Lung Screening Trial. Costs were taken from the UK Lung Cancer Screening Trial and took the perspective of the NHS and PSS. Simulants were current or former smokers aged between 55 and 80 years and so at a higher risk of lung cancer relative to the general population. Subgroups were defined by further restricting age and risk of lung cancer as predicted by patient self-questionnaire. Programme designs were single, triple, annual and biennial arrangements of LDCT screens, thereby examining number and interval length. Forty-eight distinct screening strategies were compared to the current practice of no screening. The primary outcome was incremental cost-effectiveness of strategies (additional cost per QALY gained).
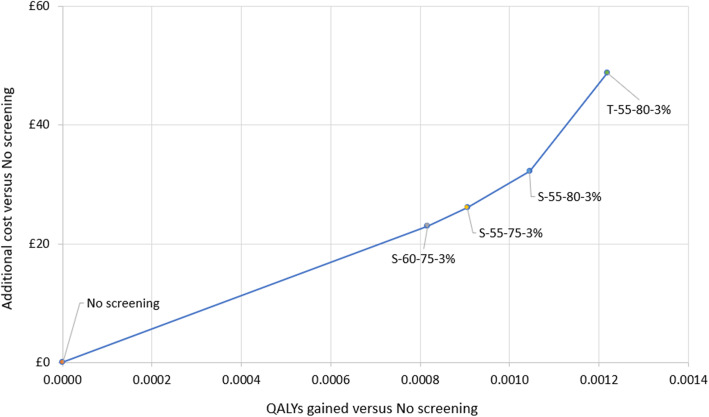
LDCT screening is predicted to bring forward the stage distribution at diagnosis and reduce lung cancer mortality, with decreases versus no screening ranging from 4.2 to 7.7% depending on screen frequency. Overall healthcare costs are predicted to increase; treatment cost savings from earlier detection are outweighed by the costs of over-diagnosis. Single-screen programmes for people 55-75 or 60-75 years with ≥ 3% predicted lung cancer risk may be cost-effective at the £30,000 per QALY threshold (respective ICERs of £28,784 and £28,169 per QALY gained). Annual and biennial screening programmes were not predicted to be cost-effective at any cost-effectiveness threshold.
LDCT performance was unaffected by lung cancer type, stage or location and the impact of a national screening programme of smoking behaviour was not included.
Lung cancer screening may not be cost-effective at the threshold of £20,000 per QALY commonly used in the UK but may be cost-effective at the higher threshold of £30,000 per QALY.
一项对肺癌经济评估的系统评价发现,没有基于疾病自然史的英国背景下的经济模型。我们首先试图开发一种用于人群筛查的自然史新模型,然后探索多种替代潜在方案的成本效益。
在MS Excel®中构建了一个个体患者模型(ENaBL),并根据美国国家肺癌筛查试验的数据进行校准。成本取自英国肺癌筛查试验,采用了英国国家医疗服务体系(NHS)和公共卫生服务(PSS)的视角。模拟对象为年龄在55至80岁之间的当前或既往吸烟者,因此相对于普通人群,他们患肺癌的风险更高。亚组是通过进一步限制年龄和根据患者自我问卷预测的患肺癌风险来定义的。方案设计包括低剂量计算机断层扫描(LDCT)筛查的单次、三次、年度和两年期安排,从而研究筛查次数和间隔时间长度。将48种不同的筛查策略与当前不进行筛查的做法进行了比较。主要结果是策略的增量成本效益(每获得一个质量调整生命年的额外成本)。
预计LDCT筛查会使诊断时的分期分布提前,并降低肺癌死亡率,与不进行筛查相比,降低幅度在4.2%至7.7%之间,具体取决于筛查频率。预计总体医疗成本会增加;早期检测带来的治疗成本节省被过度诊断的成本所抵消。对于预测肺癌风险≥3%的55至75岁或60至75岁人群,单次筛查方案在每质量调整生命年30,000英镑的阈值下可能具有成本效益(每获得一个质量调整生命年的增量成本效益比分别为28,784英镑和28,169英镑)。预计年度和两年期筛查方案在任何成本效益阈值下都不具有成本效益。
LDCT的性能不受肺癌类型、分期或位置的影响,且未纳入全国性筛查计划对吸烟行为的影响。
在英国常用的每质量调整生命年20,000英镑的阈值下,肺癌筛查可能不具有成本效益,但在每质量调整生命年30,000英镑的较高阈值下可能具有成本效益。