Brown Lynsey Rachael, Sullivan Frank, Treweek Shaun, Haddow Anne, Mountain Rodney, Selby Colin, Beusekom Mara van
School of Medicine, University of St Andrews, North Haugh, St Andrews, Scotland, UK, KY16 9TF.
Health Services Research Unit, University of Aberdeen, Foresterhill, Aberdeen, Scotland, UK, AB25 2ZD.
BMC Public Health. 2022 Apr 23;22(1):815. doi: 10.1186/s12889-022-12998-0.
Lung cancer is the most common cause of cancer death in the UK. Low-dose computed tomography (LDCT) screening has been shown to identify lung cancer at an earlier stage. A risk stratified approach to LDCT referral is recommended. Those at higher risk of developing lung cancer (aged 55 + , smoker, deprived area) are least likely to participate in such a programme and, therefore, it is necessary to understand the barriers they face and to develop pathways for implementation in order to increase uptake.
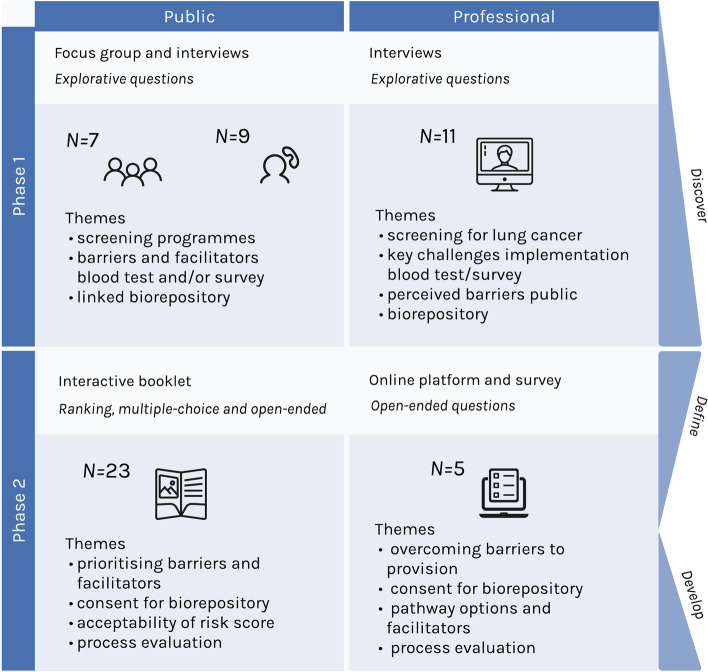
A 2-phased co-design process was employed to identify ways to further increase opportunity for uptake of a lung cancer screening programme, using a risk indicator for LDCT referral, amongst people who could benefit most. Participants were members of the public at high risk from developing lung cancer and professionals who may provide or signpost to a future lung cancer screening programme. Phase 1: interviews and focus groups, considering barriers, facilitators and pathways for provision. Phase 2: interactive offline booklet and online surveys with professionals. Qualitative data was analysed thematically, while descriptive statistics were conducted for quantitative data.
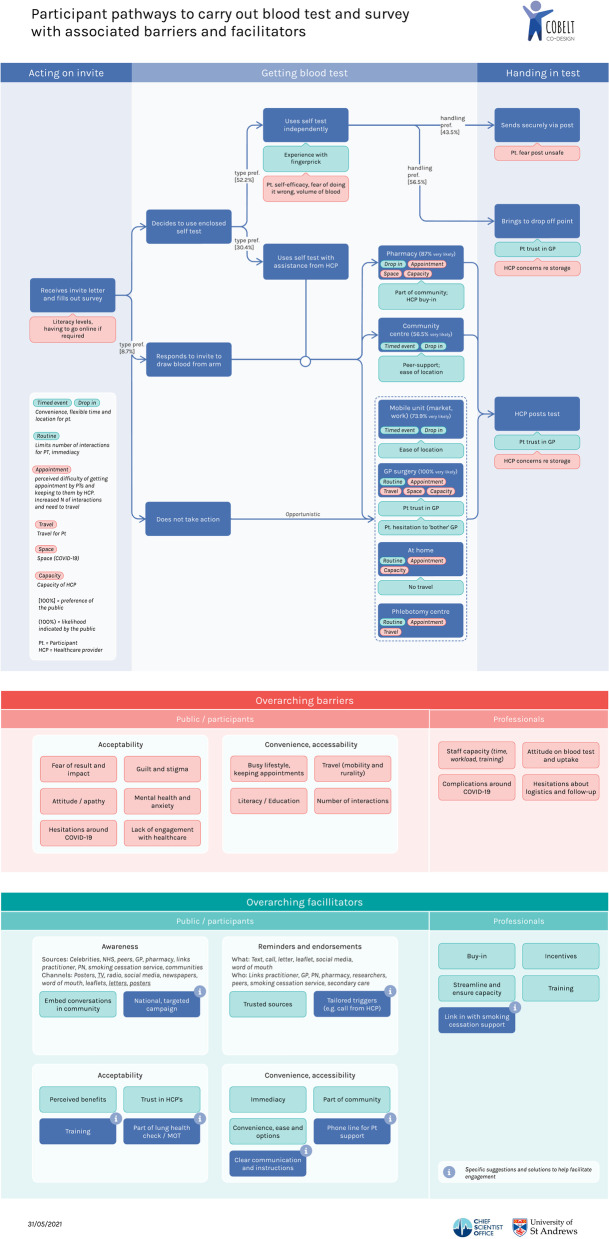
In total, ten barriers and eight facilitators to uptake of a lung cancer screening programme using a biomarker blood test for LDCT referral were identified. An additional four barriers and four facilitators to provision of such a programme were identified. These covered wider themes of acceptability, awareness, reminders and endorsement, convenience and accessibility. Various pathway options were evidenced, with choice being a key facilitator for uptake. There was a preference (19/23) for the provision of home test kits but 7 of the 19 would like an option for assistance, e.g. nurse, pharmacist or friend. TV was the preferred means of communicating about the programme and fear was the most dominant barrier perceived by members of the public.
Co-design has provided a fuller understanding of the barriers, facilitators and pathways for the provision of a future lung cancer screening programme, with a focus on the potential of biomarker blood tests for the identification of at-risk individuals. It has also identified possible solutions and future developments to enhance uptake, e.g. Embedding the service in communities, Effective communication, Overcoming barriers with options. Continuing the process to develop these solutions in a collaborative way helps to encourage the personalised approach to delivery that is likely to improve uptake amongst groups that could benefit most.
肺癌是英国癌症死亡的最常见原因。低剂量计算机断层扫描(LDCT)筛查已被证明能在更早阶段发现肺癌。建议采用风险分层方法进行LDCT转诊。那些患肺癌风险较高的人群(年龄在55岁及以上、吸烟者、贫困地区居民)参与此类项目的可能性最小,因此,有必要了解他们面临的障碍并制定实施途径,以提高参与率。
采用两阶段协同设计流程,以确定在可能受益最大的人群中,如何利用LDCT转诊风险指标进一步增加肺癌筛查项目的参与机会。参与者包括患肺癌风险高的公众以及可能提供或为未来肺癌筛查项目提供指引的专业人员。第一阶段:进行访谈和焦点小组讨论,考虑提供服务的障碍、促进因素和途径。第二阶段:与专业人员开展交互式离线手册和在线调查。对定性数据进行主题分析,对定量数据进行描述性统计。
总共确定了使用生物标志物血液检测进行LDCT转诊的肺癌筛查项目参与的10个障碍和8个促进因素。还确定了提供此类项目的另外4个障碍和4个促进因素。这些涵盖了可接受性、认知度、提醒和认可、便利性和可及性等更广泛的主题。有各种途径选项得到证实,选择是参与的关键促进因素。对于提供家庭检测试剂盒有偏好(19/23),但19人中的7人希望有辅助选项,例如护士、药剂师或朋友。电视是宣传该项目的首选方式,恐惧是公众认为最主要的障碍。
协同设计使我们更全面地了解了提供未来肺癌筛查项目的障碍、促进因素和途径,重点关注生物标志物血液检测在识别高危个体方面的潜力。它还确定了提高参与率的可能解决方案和未来发展方向,例如将服务嵌入社区、进行有效沟通、通过选项克服障碍。以协作方式继续推进这些解决方案的制定,有助于鼓励采用个性化的服务提供方式,这可能会提高最可能受益群体的参与率。