Crown Princess Victoria Children's Hospital, and Department of Biomedical and Clinical Sciences, Department of Pediatrics, Linköping University, 581 83 Linköping, Sweden.
Department of Clinical Sciences Lund, Pediatric Heart Center, Skåne University Hospital, Lund University, 221 00 Lund, Sweden.
Genes (Basel). 2020 Dec 8;11(12):1472. doi: 10.3390/genes11121472.
Sudden cardiac death (SCD) and early onset cardiomyopathy (CM) in the young will always lead to suspicion of an underlying genetic disorder. Incited by the rapid advances in genetic testing for disease we have revisited families, which previously tested "gene-negative" for familial predominantly pediatric CM, in hopes of finding a causative gene variant.
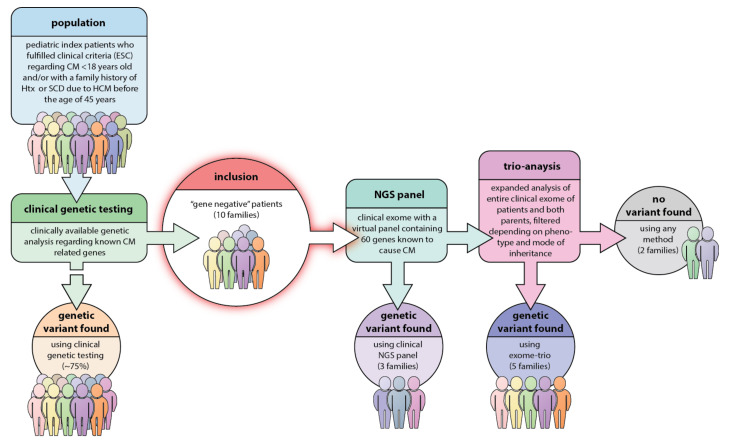
10 different families with non-syndromic pediatric CM or hypertrophic cardiomyopathy (HCM) with severe disease progression and/or heredity for HCM/CM related SCD with "gene-negative" results were included. The index patient underwent genetic testing with a recently updated gene panel for CM and SCD. In case of failure to detect a pathogenic variant in a relevant gene, the index patient and both parents underwent clinical (i.e., partial) exome sequencing (trio-exome) in order to catch pathogenic variants linked to the disease in genes that were not included in the CM panel.
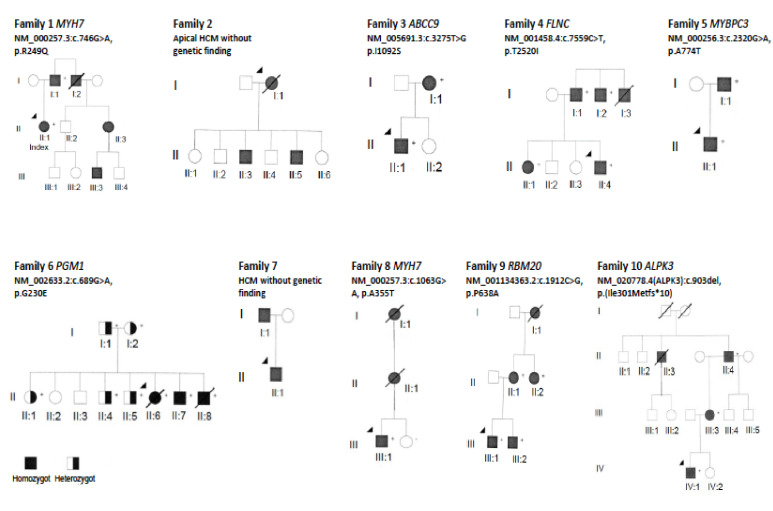
The mean age at clinical presentation of the 10 index cases was 12.5 years (boys 13.4 years, = 8; girls 9 years, = 2) and the family history burden was 33 HCM/CM cases including 9 HCM-related SCD and one heart transplantation. In 5 (50%) families we identified a genetic variant classified as pathogenic or likely pathogenic, in accordance with the American College of Medical Genetics and Genomics (ACMG) criteria, in ( = 2), , , and , respectively, and genetic variants of unknown significance (VUS) segregating with the disease in an additional 3 (30%) families, in , , and , respectively.
Our results show the importance of renewed thorough clinical assessment and the necessity to challenge previous genetic test results with more comprehensive updated gene panels or exome sequencing if the initial test failed to identify a causative gene for early onset CM or SCD in children. In pediatric cardiomyopathy cases when the gene panel still fails to detect a causative variant, a trio exome sequencing strategy might resolve some unexplained cases, especially if a multisystemic condition is clinically missed.
儿童时期的心脏性猝死(SCD)和早期起病的心肌病(CM)总是会引起对潜在遗传疾病的怀疑。受疾病基因检测快速发展的启发,我们重新检查了以前被检测为家族性主要儿科 CM“基因阴性”的家族,希望能找到致病基因变异。
10 个不同的家族患有非综合征性儿科 CM 或肥厚型心肌病(HCM),疾病进展严重,或遗传性 HCM/CM 相关 SCD“基因阴性”。索引患者接受了 CM 和 SCD 的最新基因面板的基因检测。如果在相关基因中未检测到致病变异,则索引患者和父母双方都进行了临床(即部分)外显子组测序(三重外显子组测序),以捕捉未包含在 CM 面板中的疾病相关基因中的致病变异。
10 个索引病例的临床发病年龄平均为 12.5 岁(男孩 13.4 岁,n=8;女孩 9 岁,n=2),家族史负担为 33 例 HCM/CM 病例,包括 9 例 HCM 相关 SCD 和 1 例心脏移植。在 5 个(50%)家族中,我们发现了一种符合美国医学遗传学与基因组学学院(ACMG)标准的遗传变异,分别归类为致病性或可能致病性,在、、和中,分别,以及另外 3 个(30%)家族中遗传变异的意义不明(VUS)与疾病共分离,分别在、、和中。
我们的结果表明,在儿童时期早期起病的 CM 或 SCD,如果最初的基因测试未能确定病因基因,重新进行全面的临床评估和更新更全面的基因面板或外显子组测序以挑战先前的基因测试结果非常重要。在儿科心肌病病例中,如果基因面板仍然无法检测到致病变异,三重外显子组测序策略可能会解决一些无法解释的病例,特别是如果临床上错过了多系统疾病。