Panariello Fabio, Cellini Lorenzo, Speciani Maurizio, De Ronchi Diana, Atti Anna Rita
Department of Mental Health, Local Health Authorities, Bologna, Italy.
Department of Biomedical and Neuromotor Sciences, Psychiatry, Bologna University, Bologna, Italy.
Front Psychiatry. 2020 Nov 16;11:582345. doi: 10.3389/fpsyt.2020.582345. eCollection 2020.
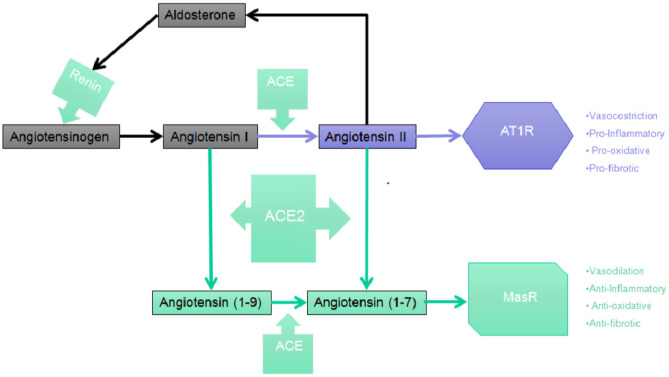
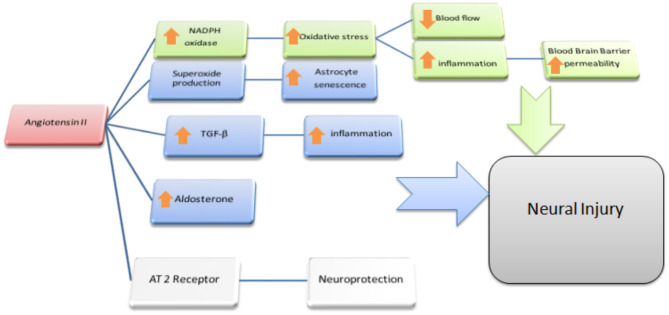
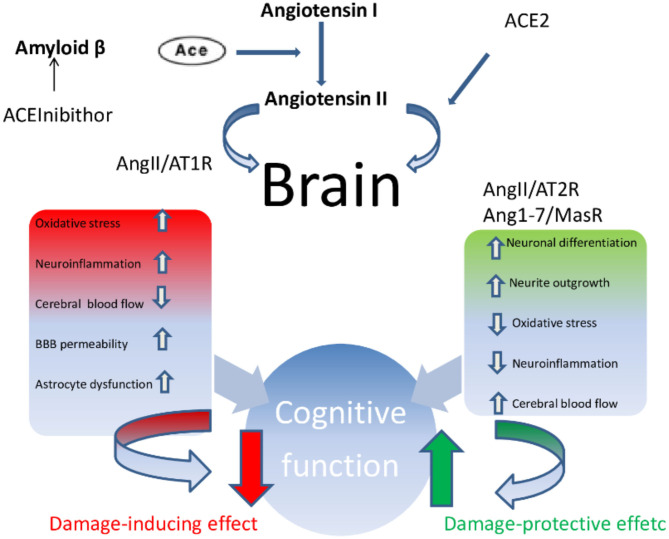
Interstitial pneumonia was the first manifestation to be recognized as caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2); however, in just a few weeks, it became clear that the coronavirus disease-2019 (COVID-19) overrun tissues and more body organs than just the lungs, so much so that it could be considered a systemic pathology. Several studies reported the involvement of the conjunctiva, the gut, the heart and its pace, and vascular injuries such as thromboembolic complications and Kawasaki disease in children and toddlers were also described. More recently, it was reported that in a sample of 214 SARS-CoV-2 positive patients, 36.4% complained of neurological symptoms ranging from non-specific manifestations (dizziness, headache, and seizures), to more specific symptoms such hyposmia or hypogeusia, and stroke. Older individuals, especially males with comorbidities, appear to be at the highest risk of developing such severe complications related to the Central Nervous System (CNS) involvement. Neuropsychiatric manifestations in COVID-19 appear to develop in patients with and without pre-existing neurological disorders. Growing evidence suggests that SARS-CoV-2 binds to the human Angiotensin-Converting Enzyme 2 (ACE2) for the attachment and entrance inside host cells. By describing ACE2 and the whole Renin Angiotensin Aldosterone System (RAAS) we may better understand whether specific cell types may be affected by SARS-CoV-2 and whether their functioning can be disrupted in case of an infection. Since clear evidences of neurological interest have already been shown, by clarifying the topographical distribution and density of ACE2, we will be able to speculate how SARS-CoV-2 may affect the CNS and what is the pathogenetic mechanism by which it contributes to the specific clinical manifestations of the disease. Based on such evidences, we finally hypothesize the process of SARS-CoV-2 invasion of the CNS and provide a possible explanation for the onset or the exacerbation of some common neuropsychiatric disorders in the elderly including cognitive impairment and Alzheimer disease.
间质性肺炎是最早被认为由严重急性呼吸综合征冠状病毒2(SARS-CoV-2)引起的表现;然而,仅仅几周后,就清楚地发现2019冠状病毒病(COVID-19)侵袭的组织和身体器官不仅仅是肺部,以至于它可被视为一种全身性病理状态。多项研究报告了结膜、肠道、心脏及其节律受累情况,还描述了儿童和幼儿的血管损伤,如血栓栓塞并发症和川崎病。最近,有报道称在214例SARS-CoV-2阳性患者样本中,36.4%的患者主诉有神经症状,范围从非特异性表现(头晕、头痛和癫痫发作)到更具体的症状,如嗅觉减退或味觉减退以及中风。老年人,尤其是患有合并症的男性,似乎发生与中枢神经系统(CNS)受累相关的此类严重并发症的风险最高。COVID-19中的神经精神表现似乎在有或没有既往神经疾病的患者中都会出现。越来越多的证据表明,SARS-CoV-2与人血管紧张素转换酶2(ACE2)结合以附着并进入宿主细胞。通过描述ACE2和整个肾素血管紧张素醛固酮系统(RAAS),我们可能会更好地理解特定细胞类型是否可能受到SARS-CoV-2影响,以及在感染情况下它们的功能是否会被破坏。由于已经有明确的神经学相关证据,通过阐明ACE2的拓扑分布和密度,我们将能够推测SARS-CoV-2如何影响中枢神经系统以及它导致该疾病特定临床表现的发病机制是什么。基于这些证据,我们最终推测SARS-CoV-2侵入中枢神经系统的过程,并为老年人中一些常见神经精神疾病(包括认知障碍和阿尔茨海默病)的发病或加重提供一种可能的解释。