Rahimy Elham, Koong Amanda, Toesca Diego, White Maya N, Panjwani Neil, Fisher George, Chang Daniel, Pollom Erqi
Department of Radiation Oncology, Stanford University, Palo Alto, California.
Department of Oncology, Stanford University, Palo Alto, California.
Adv Radiat Oncol. 2020 May 21;5(6):1188-1196. doi: 10.1016/j.adro.2020.05.001. eCollection 2020 Nov-Dec.
Our purpose was to report outcomes of elderly patients who underwent definitive treatment involving radiation therapy for esophageal cancer at our institution.
We performed a retrospective review of patients aged ≥75 years with esophageal cancer treated with definitive radiation therapy (≥45 Gy) at our institution from 1997 to 2019. Acute and late Radiation Therapy Oncology Group grade 3+ toxicities were recorded. Survival was estimated using the Kaplan-Meier method.
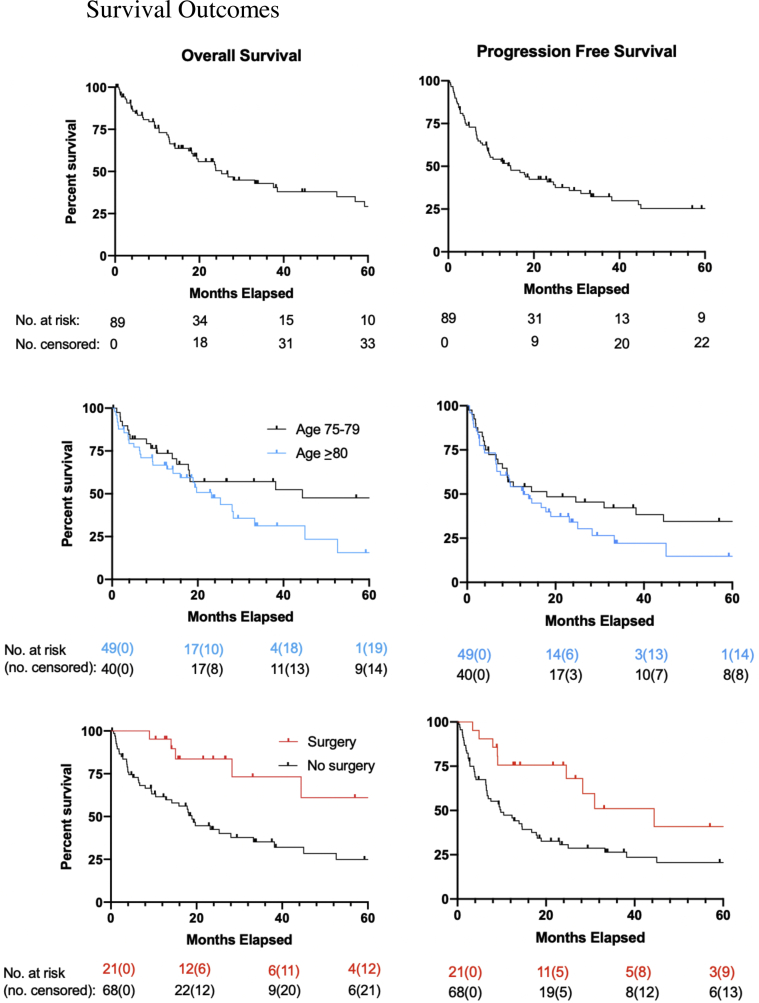
Of the 89 patients included, median age was 80 and 78% were male. Median adjusted Charlson Comorbidity Index and Karnofsky Performance Status were 5 (3-12) and 80 (50-100), respectively. The majority of cancers were adenocarcinoma (58%), distal (67%), and stage III (62%). Fifty-eight percent underwent definitive chemoradiotherapy, and one-third underwent preoperative intent chemoradiotherapy. Median prescribed dose was 50 Gy (45-66 Gy), and intensity modulated radiation therapy was used in 76%. Eighty-five percent completed the radiation therapy course. Among these, 20% had radiation therapy breaks. For those receiving concurrent chemotherapy, 37% had a dose reduction and 39.5% had a break/cycle reduction. Acute grade 3+ toxicity was 22%, with 2% grade 5 toxicity. Twenty-one of the 29 patients (72%) treated with preoperative intent underwent surgery. There were no deaths 90 days postoperatively. For patients who underwent surgery, 1- and 2-year overall survival were 95% and 84%. For those who did not undergo surgery, 1- and 2-year overall survival were 70% and 52%.
There is a role for aggressive radiation therapy in well-selected elderly patients with esophageal cancer. However, optimization of supportive care, chemotherapy regimens, radiation therapy dose/fractionation, and surgical indications are needed to reduce toxicity.
我们的目的是报告在我院接受食管癌根治性放射治疗的老年患者的治疗结果。
我们对1997年至2019年在我院接受根治性放射治疗(≥45 Gy)的年龄≥75岁的食管癌患者进行了回顾性研究。记录急性和晚期放射治疗肿瘤学组3级及以上毒性反应。采用Kaplan-Meier法估计生存率。
纳入的89例患者中,中位年龄为80岁,78%为男性。调整后的Charlson合并症指数和卡诺夫斯基功能状态评分中位数分别为5(3-12)和80(50-100)。大多数癌症为腺癌(58%),位于远端(67%),且为Ⅲ期(62%)。58%的患者接受了根治性同步放化疗,三分之一的患者接受了术前同步放化疗。处方剂量中位数为50 Gy(45-66 Gy),76%的患者采用调强放射治疗。85%的患者完成了放射治疗疗程。其中,20%的患者有放疗中断。在接受同步化疗的患者中,37%的患者减少了剂量,39.5%的患者减少了疗程。急性3级及以上毒性反应发生率为22%,5级毒性反应发生率为2%。29例接受术前同步放化疗的患者中有21例(72%)接受了手术。术后90天无死亡病例。接受手术的患者1年和2年总生存率分别为95%和84%。未接受手术的患者1年和2年总生存率分别为70%和52%。
对于精心挑选的老年食管癌患者,积极的放射治疗有一定作用。然而,需要优化支持治疗、化疗方案、放射治疗剂量/分割以及手术指征以降低毒性反应。