Research & Evaluation Kaiser Permanente Southern California Pasadena CA.
Kaiser Permanente Bernard J. Tyson School of Medicine Pasadena CA.
J Am Heart Assoc. 2021 Feb 2;10(3):e019669. doi: 10.1161/JAHA.120.019669. Epub 2020 Dec 14.
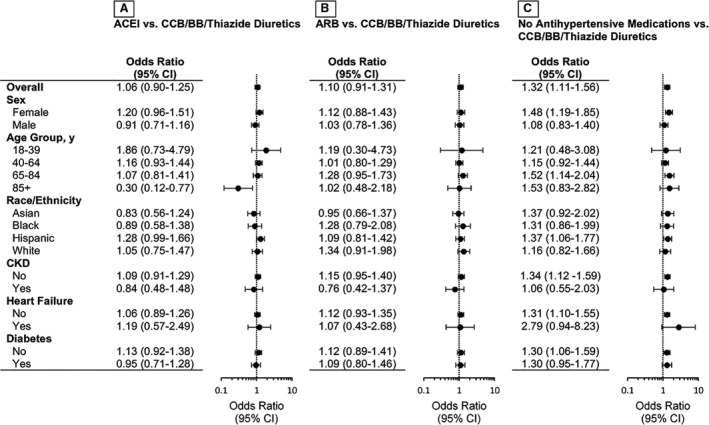
Background Previous reports suggest that the use of angiotensin-converting enzyme inhibitors (ACEIs) or angiotensin receptor blockers (ARBs) may upregulate angiotensin-converting enzyme 2 receptors and increase severe acute respiratory syndrome coronavirus 2 infectivity. We evaluated the association between ACEI or ARB use and coronavirus disease 2019 (COVID-19) infection among patients with hypertension. Methods and Results We identified patients with hypertension as of March 1, 2020 (index date) from Kaiser Permanente Southern California. Patients who received ACEIs, ARBs, calcium channel blockers, beta blockers, thiazide diuretics (TD), or no therapy were identified using outpatient pharmacy data covering the index date. Outcome of interest was a positive reverse transcription polymerase chain reaction test for COVID-19 between March 1 and May 6, 2020. Patient sociodemographic and clinical characteristics were identified within 1 year preindex date. Among 824 650 patients with hypertension, 16 898 (2.0%) were tested for COVID-19. Of those tested, 1794 (10.6%) had a positive result. Overall, exposure to ACEIs or ARBs was not statistically significantly associated with COVID-19 infection after propensity score adjustment (odds ratio [OR], 1.06; 95% CI, 0.90-1.25) for ACEIs versus calcium channel blockers/beta blockers/TD; OR, 1.10; 95% CI, 0.91-1.31 for ARBs versus calcium channel blockers/beta blockers/TD). The associations between ACEI use and COVID-19 infection varied in different age groups (-interaction=0.03). ACEI use was associated with lower odds of COVID-19 among those aged ≥85 years (OR, 0.30; 95% CI, 0.12-0.77). Use of no antihypertensive medication was significantly associated with increased odds of COVID-19 infection compared with calcium channel blockers/beta blockers/TD (OR, 1.32; 95% CI, 1.11-1.56). Conclusions Neither ACEI nor ARB use was associated with increased likelihood of COVID-19 infection. Decreased odds of COVID-19 infection among adults ≥85 years using ACEIs warrants further investigation.
先前的报告表明,血管紧张素转换酶抑制剂(ACEI)或血管紧张素受体阻滞剂(ARB)的使用可能上调血管紧张素转换酶 2 受体并增加严重急性呼吸综合征冠状病毒 2 的感染性。我们评估了高血压患者中 ACEI 或 ARB 使用与 2019 年冠状病毒病(COVID-19)感染之间的关联。
我们从 Kaiser Permanente Southern California 确定了截至 2020 年 3 月 1 日(索引日期)的高血压患者。使用门诊药房数据确定了在索引日期前 1 年内接受 ACEI、ARB、钙通道阻滞剂、β受体阻滞剂、噻嗪类利尿剂(TD)或未接受治疗的患者。感兴趣的结果是在 2020 年 3 月 1 日至 5 月 6 日之间进行的 COVID-19 逆转录聚合酶链反应检测呈阳性。在索引日期前 1 年内确定了患者的社会人口统计学和临床特征。在 824650 名高血压患者中,有 16898 人(2.0%)接受了 COVID-19 检测。在接受检测的患者中,有 1794 人(10.6%)的检测结果为阳性。总体而言,在倾向评分调整后,ACEI 或 ARB 的暴露与 COVID-19 感染没有统计学上的显著相关性(ACEI 与钙通道阻滞剂/β受体阻滞剂/TD 相比,比值比 [OR],1.06;95%置信区间,0.90-1.25);与钙通道阻滞剂/β受体阻滞剂/TD 相比,ARB 的 OR 为 1.10;95%置信区间,0.91-1.31)。ACEI 与 COVID-19 感染之间的关联在不同年龄组中存在差异(-交互作用=0.03)。ACEI 与 85 岁及以上人群 COVID-19 感染的可能性降低相关(OR,0.30;95%置信区间,0.12-0.77)。与钙通道阻滞剂/β受体阻滞剂/TD 相比,不使用任何降压药物与 COVID-19 感染的可能性增加显著相关(OR,1.32;95%置信区间,1.11-1.56)。
ACEI 和 ARB 的使用均与 COVID-19 感染的可能性增加无关。85 岁及以上使用 ACEI 的成年人 COVID-19 感染可能性降低值得进一步研究。