Knight Cardiovascular Institute, Oregon Health and Science University, Portland, Oregon.
Knight Cardiovascular Institute, Oregon Health and Science University, Portland, Oregon.
Am J Cardiol. 2022 Feb 15;165:101-108. doi: 10.1016/j.amjcard.2021.10.050. Epub 2021 Dec 11.
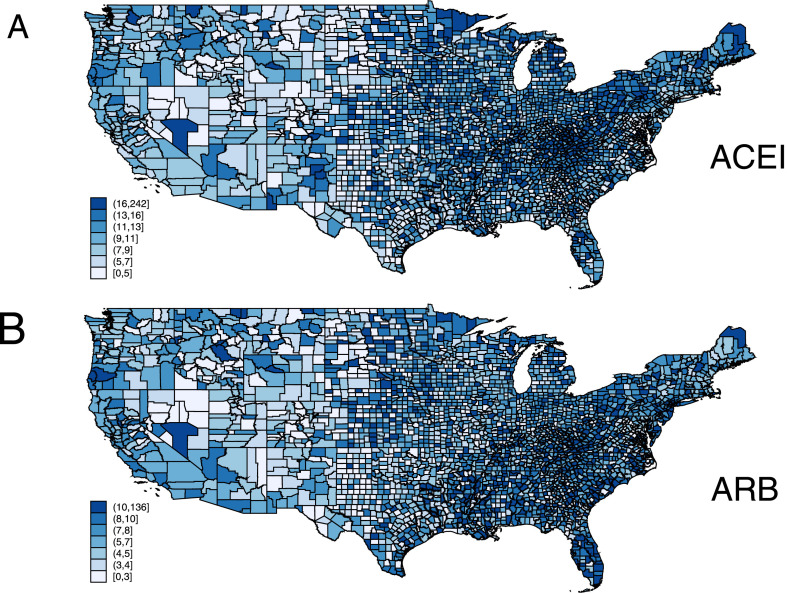
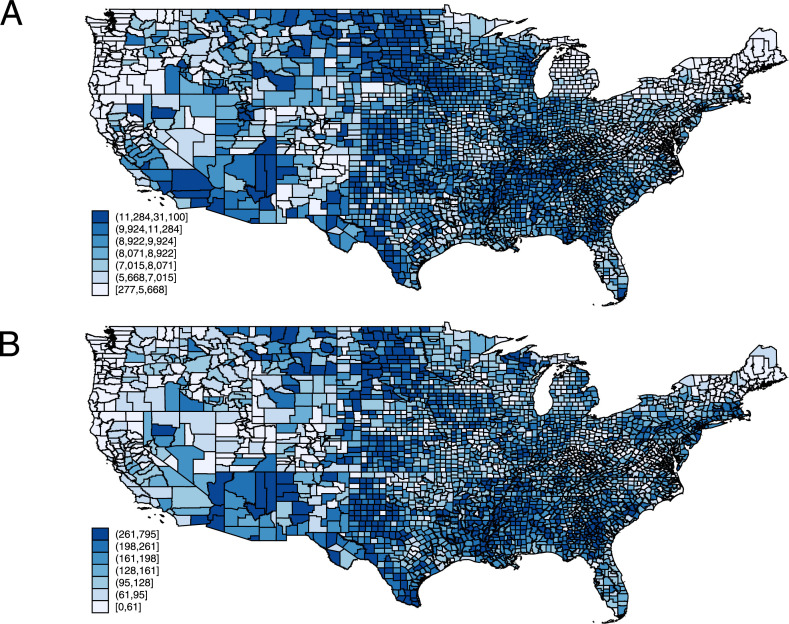
The novel coronavirus SARS-CoV-2 uses the angiotensin-converting enzyme 2 receptor as an entry point to the cell. Cardiovascular disease (CVD) is a risk factor for COVID-19 with poor outcomes. We tested the hypothesis that the rate of angiotensin-converting enzyme inhibitor (ACEI) and angiotensin receptor blocker (ARB) use is associated with the rate of COVID-19-confirmed cases and deaths. We conducted a geospatial, ecological study using publicly available county-level data. The Medicare ACEI and ARB prescription rate was exposure. The COVID-19-confirmed case and death rates were outcomes. Spatial autoregression models were adjusted for the rate of births and deaths; Group Quarters population; percentage of female; percentage of Native American, Pacific Islander, Hispanic, and Black; percentage of children and older (>65 years) adults; percentage of uninsured; percentage of those living in poverty; percentage of those who are obese, smoking, admitting insufficient sleep, and those with at least some college degree; median household income; air quality index; CVD hospitalization rate in Medicare beneficiaries; and CVD death rate in a total county population. After adjustment for confounders, the ACEI use rate did not associate with COVID-19-confirmed case rate (direct county-own effect + 0.027%; 95% confidence interval [CI] -1.080 to 1.134; p = 0.962; indirect spillover effect + 0.26%; 95% CI -70.0 to 70.5; p = 0.994). Similarly, the ARB use rate was not associated with COVID-19-confirmed case rate (direct effect + 0.029%; 95% CI -0.803 to 0.862; p = 0.945; indirect effect + 0.19%; 95% CI -52.8 to 53.2; p = 0.994). In both unadjusted and adjusted Bayesian zero inflation Poisson analysis, neither ACEI nor ARB use rates were associated with COVID-19 death rates. In conclusion, ACEI and ARB use rates were not associated with COVID-19 infectivity and death rate in this ecological study.
新型冠状病毒 SARS-CoV-2 使用血管紧张素转化酶 2 受体作为进入细胞的入口。心血管疾病(CVD)是 COVID-19 的危险因素,预后不良。我们检验了以下假设,即血管紧张素转换酶抑制剂(ACEI)和血管紧张素受体阻滞剂(ARB)的使用率与 COVID-19 确诊病例和死亡人数有关。我们使用公开的县级数据进行了地理空间、生态研究。医疗保险 ACEI 和 ARB 处方率为暴露因素。COVID-19 确诊病例和死亡率为结果。空间自回归模型调整了出生率和死亡率;群体居住人口;女性比例;美洲原住民、太平洋岛民、西班牙裔和非裔美国人比例;儿童和 65 岁以上成年人比例;未参保比例;贫困人口比例;肥胖、吸烟、睡眠不足和至少有一些大学学历的比例;家庭中位数收入;空气质量指数;医疗保险受益人中的 CVD 住院率;以及全县总人口中的 CVD 死亡率。在调整混杂因素后,ACEI 使用率与 COVID-19 确诊病例率无关(直接县自有效应+0.027%;95%置信区间[CI] -1.080 至 1.134;p=0.962;间接溢出效应+0.26%;95%CI -70.0 至 70.5;p=0.994)。同样,ARB 使用率与 COVID-19 确诊病例率无关(直接效应+0.029%;95%CI -0.803 至 0.862;p=0.945;间接效应+0.19%;95%CI -52.8 至 53.2;p=0.994)。在未调整和调整后的贝叶斯零膨胀泊松分析中,ACEI 和 ARB 的使用率均与 COVID-19 死亡率无关。总之,在这项生态研究中,ACEI 和 ARB 的使用率与 COVID-19 的传染性和死亡率无关。