Tuominen Jalmari, Hällberg Ville, Oksala Niku, Palomäki Ari, Lukkarinen Timo, Roine Antti
Faculty of Medicine and Life Sciences, Tampere University, Tampere, Finland.
Emergency Department, Kanta-Häme Central Hospital, Hämeenlinna, Finland.
BMC Emerg Med. 2020 Dec 11;20(1):97. doi: 10.1186/s12873-020-00392-1.
Emergency departments (EDs) worldwide have been in the epicentre of the novel coronavirus disease (COVID-19). However, the impact of the pandemic and national emergency measures on the number of non-COVID-19 presentations and the assessed acuity of those presentations remain uncertain.
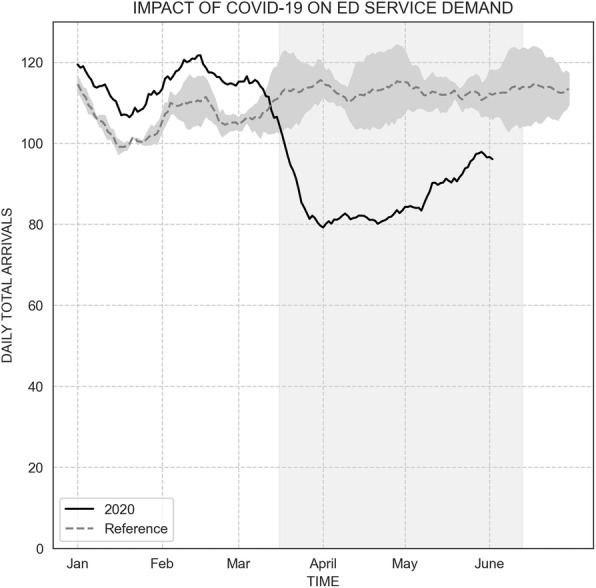
We acquired a retrospective cohort containing all ED visits in a Finnish secondary care hospital during years 2018, 2019 and 2020. We compared the number of presentations in 2020 during the national state of emergency, i.e. from March 16 to June 11, with numbers from 2018 and 2019. Presentations were stratified using localized New York University Emergency Department Algorithm (NYU-EDA) to evaluate changes in presentations with different acuity levels.
A total of 27,526 presentations were observed. Compared to previous two years, total daily presentations were reduced by 23% (from 113 to 87, p < .001). In NYU-EDA classes, Non-Emergent visits were reduced the most by 42% (from 18 to 10, p < .001). Emergent presentations were reduced by 19 to 28% depending on the subgroup (p < .001). Number of injuries were reduced by 25% (from 27 to 20, p < .001). The NYU-EDA distribution changed statistically significantly with 4% point reduction in Non-Emergent visits (from 16 to 12%, p < .001) and 0.9% point increase in Alcohol-related visits (from 1.6 to 2.5%, p < .001).
We observed a significant reduction in total ED visits in the course of national state of emergency. Presentations were reduced in most of the NYU-EDA groups irrespective of the assessed acuity. A compensatory increase in presentations was not observed in the course of the 3 month lockdown. This implies either reduction in overall morbidity caused by decreased societal activity or widespread unwillingness to seek required medical advice.
世界各地的急诊科一直处于新型冠状病毒肺炎(COVID-19)疫情的中心。然而,疫情和国家紧急措施对非COVID-19就诊人数及其评估的严重程度的影响仍不确定。
我们获取了一个回顾性队列,其中包含芬兰一家二级护理医院在2018年、2019年和2020年期间的所有急诊科就诊记录。我们将2020年国家紧急状态期间(即3月16日至6月11日)的就诊人数与2018年和2019年的人数进行了比较。使用本地化的纽约大学急诊科算法(NYU-EDA)对就诊情况进行分层,以评估不同严重程度就诊情况的变化。
共观察到27526次就诊。与前两年相比,每日就诊总数减少了23%(从113次降至87次,p < 0.001)。在NYU-EDA分类中,非紧急就诊减少最多,减少了42%(从18次降至10次,p < 0.001)。紧急就诊根据亚组不同减少了19%至28%(p < 0.001)。受伤人数减少了25%(从27人降至20人,p < 0.001)。NYU-EDA分布有统计学显著变化,非紧急就诊减少了4个百分点(从16%降至12%,p < 0.001),与酒精相关的就诊增加了0.9个百分点(从1.6%升至2.5%,p < 0.001)。
我们观察到在国家紧急状态期间急诊科就诊总数显著减少。在大多数NYU-EDA组中,无论评估的严重程度如何,就诊人数都有所减少。在3个月的封锁期间未观察到就诊人数的代偿性增加。这意味着社会活动减少导致总体发病率降低,或者普遍不愿意寻求所需的医疗建议。