Department of Health Law, Policy, and Management, Boston University School of Public Health, Boston, Massachusetts.
Section of Infectious Diseases, Department of Medicine, Boston Medical Center, Boston, Massachusetts.
JAMA Netw Open. 2020 Dec 1;3(12):e2029676. doi: 10.1001/jamanetworkopen.2020.29676.
Whereas outpatient treatment with medication for opioid use disorder (MOUD) is evidence based, there is a large network of inpatient facilities in the US that are reimbursed by commercial insurers and do not typically offer MOUD.
To compare the rates of opioid-related overdose and all-cause hospitalization after outpatient MOUD treatment vs inpatient care.
DESIGN, SETTING, AND PARTICIPANTS: This comparative effectiveness research study used deidentified claims of commercially insured individuals in the US from the MarketScan Commercial Claims and Encounters Database from January 1, 2010, to December 31, 2017, to obtain a sample of 37 090 individuals with opioid use disorder who initiated treatment with inpatient care and/or MOUD. Data were analyzed from October 1, 2019, to May 1, 2020. To address nonrandom treatment assignment, individuals with opioid use disorder who initiated MOUD or who entered inpatient care were matched 1:1 based on propensity scores.
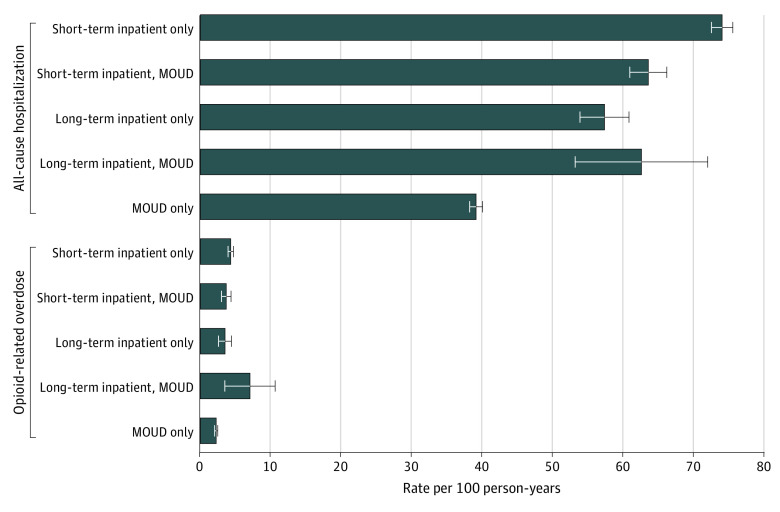
The independent variable of interest was the type of treatment initiated. Individuals could initiate 1 of 5 potential treatments: (1) outpatient MOUD, (2) short-term inpatient care, (3) short-term inpatient care followed by outpatient MOUD within 30 days, (4) long-term inpatient care, or (5) long-term inpatient care followed by outpatient MOUD within 30 days.
Opioid-related overdose and all-cause hospitalization at any point within the 12 months after treatment of opioid use disorder. The hazard for each outcome was estimated using a time-to-event Cox proportional hazards regression model.
The cohort included 37 090 individuals matched 1:1 between inpatient and outpatient treatment (20 723 [56%] were younger than 30 years; 23 250 [63%] were male). After propensity score matching, compared with the inpatient treatments, initiation of outpatient MOUD alone was followed by the lowest 1-year overdose rate (2.2 [95% CI, 2.0-2.5] per 100 person-years vs 3.5 [95% CI, 2.7-4.4] to 7.0 [95% CI, 4.6-10.7] per 100 person-years) and hospitalization rate (39 [95% CI, 38-40] per 100 person-years vs 57 [95% CI, 54-61] to 74 [95% CI, 73-76] per 100 person-years). Outpatient MOUD was also associated with the lowest hazard of these events compared with inpatient care, which had hazard ratios ranging from 1.71 (95% CI, 1.35-2.17) to 2.67 (95% CI, 1.68-4.23) for overdose and 1.33 (95% CI, 1.23-1.44) to 1.90 (95% CI, 1.83-1.97) for hospitalizations.
The results of this comparative effectiveness research study suggest that lower rates of subsequent overdose and hospitalization are associated with outpatient MOUD compared with short- or long-term inpatient care. When patients and clinicians have a choice of treatment, outpatient MOUD treatment may be associated with lower overdose and hospitalization on balance. Future research should assess which patients benefit most from inpatient care and how best to leverage existing inpatient treatment infrastructure.
尽管门诊药物治疗阿片类药物使用障碍(MOUD)是有证据支持的,但美国有大量的住院设施通过商业保险公司获得补偿,且通常不提供 MOUD。
比较门诊 MOUD 治疗与住院治疗后阿片类药物相关药物过量和全因住院的发生率。
设计、地点和参与者:这项基于人群的比较有效性研究使用了美国市场扫描商业索赔和就诊数据库中的商业保险个人的匿名索赔数据,时间范围为 2010 年 1 月 1 日至 2017 年 12 月 31 日,纳入了 37090 名患有阿片类药物使用障碍并开始接受住院或 MOUD 治疗的个体。数据于 2019 年 10 月 1 日至 2020 年 5 月 1 日进行分析。为了解决非随机治疗分配问题,开始接受 MOUD 或住院治疗的阿片类药物使用障碍个体根据倾向评分进行 1:1 匹配。
感兴趣的独立变量是治疗的类型。个体可以接受以下 5 种治疗中的 1 种:(1)门诊 MOUD;(2)短期住院治疗;(3)30 天内短期住院治疗后接受门诊 MOUD;(4)长期住院治疗;(5)30 天内长期住院治疗后接受门诊 MOUD。
治疗后 12 个月内任何时间发生的阿片类药物相关药物过量和全因住院。使用时间到事件 Cox 比例风险回归模型估计每种结局的风险。
该队列包括 37090 名个体,1:1 匹配住院和门诊治疗(20723 名[56%]年龄小于 30 岁;23250 名[63%]为男性)。在倾向评分匹配后,与住院治疗相比,单独使用门诊 MOUD 后 1 年的药物过量发生率最低(2.2 [95% CI,2.0-2.5]/100 人年,而 3.5 [95% CI,2.7-4.4]至 7.0 [95% CI,4.6-10.7]/100 人年)和住院率最低(39 [95% CI,38-40]/100 人年,而 57 [95% CI,54-61]至 74 [95% CI,73-76]/100 人年)。与住院治疗相比,门诊 MOUD 也与这些事件的最低风险相关,药物过量的风险比为 1.71(95% CI,1.35-2.17)至 2.67(95% CI,1.68-4.23),住院的风险比为 1.33(95% CI,1.23-1.44)至 1.90(95% CI,1.83-1.97)。
这项基于人群的比较有效性研究的结果表明,与短期或长期住院治疗相比,门诊 MOUD 治疗与随后药物过量和住院的发生率较低相关。当患者和临床医生有治疗选择时,门诊 MOUD 治疗可能总体上与较低的药物过量和住院相关。未来的研究应评估哪些患者从住院治疗中获益最大,以及如何最好地利用现有的住院治疗基础设施。