Rössling Rosa, Prüss Harald
Department of Neurology and Experimental Neurology, Charité - Universitätsmedizin Berlin, CharitéCrossOver, R 4-334 ,Charitéplatz 1, 10117 Berlin, Germany.
German Center for Neurodegenerative Diseases (DZNE) Berlin, Berlin, Germany.
Neurol Res Pract. 2020 Jan 15;2:1. doi: 10.1186/s42466-019-0048-7. eCollection 2020.
Antibody-mediated and paraneoplastic autoimmune encephalitides (AE) present with a broad spectrum of clinical symptoms. They often lead to progressing inflammatory changes of the central nervous system with subacute onset and can cause persistent brain damage. Thus, to promptly start the appropriate and AE-specific therapy, recognition of symptoms, initiation of relevant antibody diagnostics and confirmation of the clinical diagnosis are crucial, in particular as the diseases are relatively rare.
This standard operating procedure (SOP) should draw attention to the clinical presentation of AE, support the diagnostic approach to patients with suspected AE and guide through the necessary steps including therapeutic decisions, tumour screening and exclusion of differential diagnoses.
Based on existing diagnostic algorithms, treatment recommendations and personal experiences, this SOP gives an overview of clinical presentation, diagnostic procedures and therapy in AE. Additional information is provided within an accompanying text and a table describing the most important autoantibodies and their characteristics.
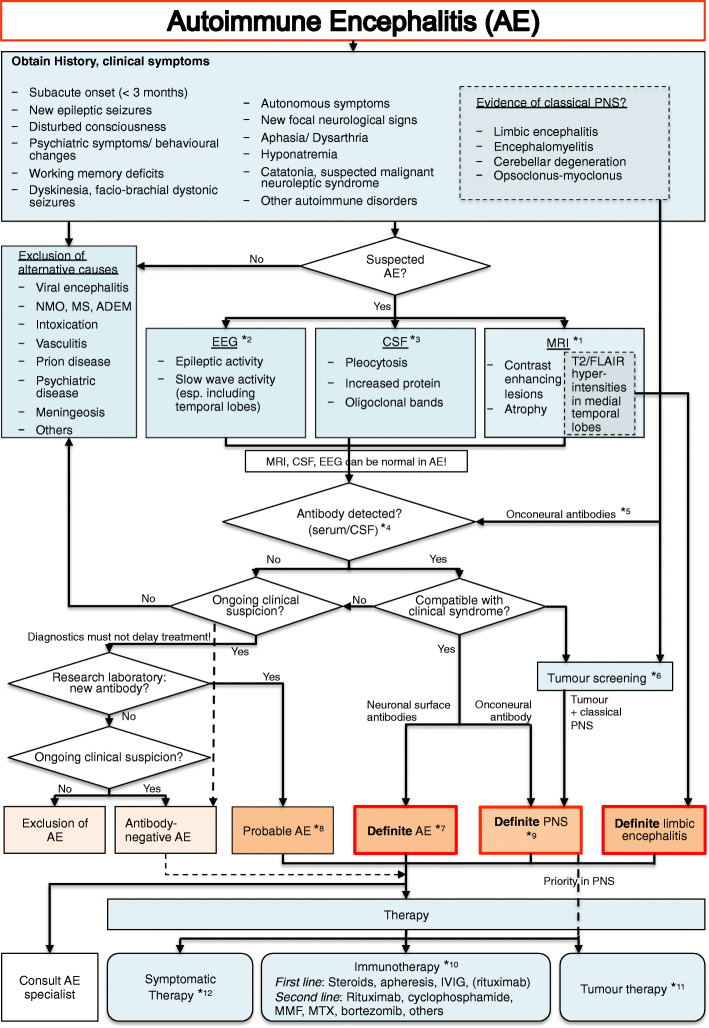
The initial steps of the AE flow chart are based on clinical symptoms and the patient's history. Assignment to paraneoplastic or antibody-mediated AE is sometimes clinically possible. Diagnostics should include MRI, EEG and CSF analysis with antibody panel diagnostic. Definite AE can be diagnosed if the underlying antibody is compatible with the clinical presentation. Classification of probable AE may be possible even with negative anti-neuronal autoantibodies if the clinical presentation and laboratory abnormalities are highly suggestive of AE. The confirmed AE diagnosis requires immediate initiation of immunotherapy.
The SOP facilitates the recognition of patients with AE and presents the necessary diagnostic and therapeutic steps.
抗体介导的副肿瘤性自身免疫性脑炎(AE)具有广泛的临床症状。它们常导致中枢神经系统进行性炎症改变,起病亚急性,可造成持续性脑损伤。因此,为及时启动恰当的、针对AE的治疗,识别症状、启动相关抗体诊断及确认临床诊断至关重要,尤其是鉴于这些疾病相对罕见。
本标准操作程序(SOP)应关注AE的临床表现,支持对疑似AE患者的诊断方法,并指导必要步骤,包括治疗决策、肿瘤筛查及排除鉴别诊断。
基于现有的诊断算法、治疗建议及个人经验,本SOP概述了AE的临床表现、诊断程序及治疗。在随附文本及描述最重要自身抗体及其特征的表格中提供了更多信息。
AE流程图的初始步骤基于临床症状和患者病史。有时临床上可将其归为副肿瘤性或抗体介导的AE。诊断应包括MRI、脑电图(EEG)及脑脊液(CSF)分析和抗体谱诊断。如果潜在抗体与临床表现相符,则可确诊AE。如果临床表现和实验室异常高度提示AE,即使抗神经元自身抗体阴性,也可能进行可能的AE分类。确诊AE诊断后需立即启动免疫治疗。
本SOP有助于识别AE患者,并呈现必要的诊断和治疗步骤。