Pilbery Richard, Miles Jamie, Bell Fiona
Yorkshire Ambulance Service NHS Trust: ORCID iD: https://orcid.org/0000-0002-5797-9788.
Yorkshire Ambulance Service NHS Trust: ORCID iD: https://orcid.org/0000-0002-1080-768X.
Br Paramed J. 2019 Sep 1;4(2):37-45. doi: 10.29045/14784726.2019.09.4.2.37.
Evidence from the past 20 years has highlighted that acute pain is not managed well in the emergency setting, in particular with children. Inadequate management of pain can result in long-term changes in both physical and mental health. This service evaluation aimed to determine how paediatric pain is assessed and managed by ambulance clinicians in a large region in England.
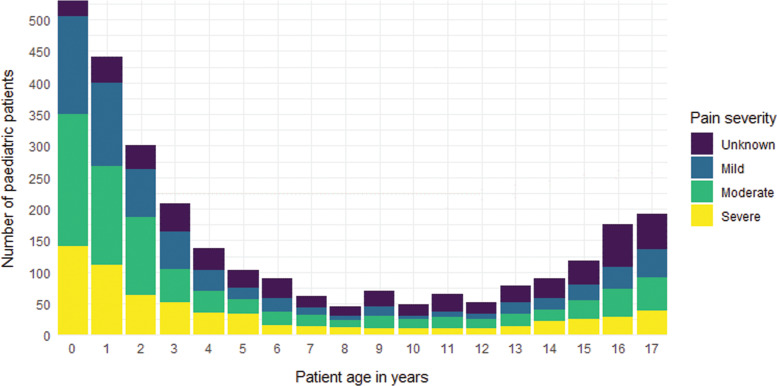
This retrospective service evaluation analysed electronic patient record (ePR) data routinely collected between September and December 2018. All paediatric patients (< 18 years of age) with pain documented narratively, or a pain score of ≥ 1/10, were included. The primary outcome measure was the proportion of patients with severe pain (defined as a pain score of ≥ 7/10) who achieve effective pain management (reduction in pain score of ≥ 2/10).
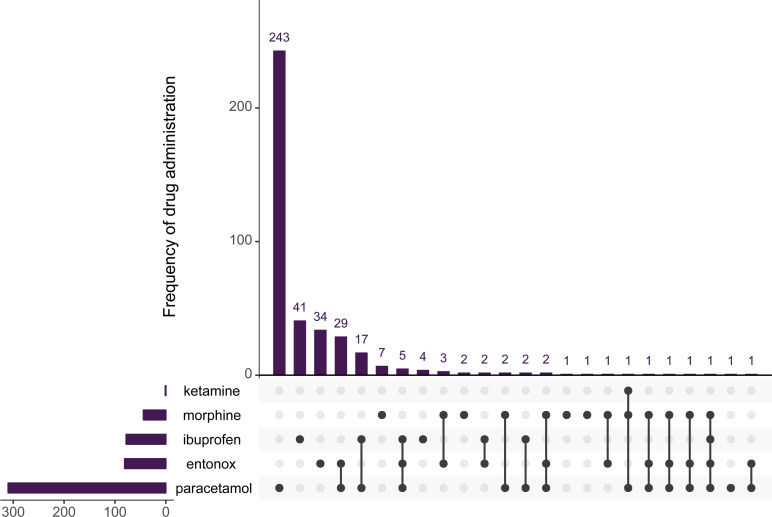
A total of 2801 paediatric patients who had documented pain were included in the analysis and the median age of patients was three years (interquartile range, 1-12 years). Most had a medical cause of pain (2387/2801, 85.2%), and analgesia was administered by the ambulance crew in 403/2801 (14.4%) patients. Multiple pain scores were recorded for 667 patients. Effective pain management was achieved in 233/271 (86%) patients in moderate pain and 204/210 (97.1%) patients in severe pain. However, of the 437 children in moderate to severe pain who achieved effective pain management, 381 (87%) received no analgesia.
Children in severe pain received effective pain management, despite the majority not receiving any analgesia. This should be investigated further since non-pharmacological methods of analgesia are unlikely to explain a reduction of this magnitude. Ambulance staff need to be encouraged to record a pain score promptly after arriving on scene and ensure it is repeated. Pain score should be documented as part of the physiological observations and not in the free text of ePRs to ensure that it is identified during audits.
过去20年的证据表明,急诊环境下的急性疼痛,尤其是儿童的急性疼痛,未得到妥善处理。疼痛管理不当会导致身心健康的长期变化。这项服务评估旨在确定英格兰一个大区域的救护车临床医生如何评估和管理儿童疼痛。
这项回顾性服务评估分析了2018年9月至12月期间常规收集的电子病历(ePR)数据。纳入所有有疼痛描述记录或疼痛评分≥1/10的儿科患者(<18岁)。主要结局指标是达到有效疼痛管理(疼痛评分降低≥2/10)的重度疼痛患者(定义为疼痛评分≥7/10)的比例。
共有2801名有疼痛记录的儿科患者纳入分析,患者的中位年龄为3岁(四分位间距,1 - 12岁)。大多数患者的疼痛有医学原因(2387/2801,85.2%),403/2801(14.4%)的患者由救护人员给予了镇痛治疗。667名患者记录了多个疼痛评分。中度疼痛的233/271(86%)患者和重度疼痛的204/210(97.1%)患者实现了有效疼痛管理。然而,在437名实现有效疼痛管理的中度至重度疼痛儿童中,381名(87%)未接受任何镇痛治疗。
重度疼痛的儿童实现了有效疼痛管理,尽管大多数未接受任何镇痛治疗。鉴于非药物镇痛方法不太可能解释如此程度的疼痛减轻,这一现象应进一步调查。需要鼓励救护人员在到达现场后立即记录疼痛评分,并确保重复记录。疼痛评分应作为生理观察的一部分记录,而不是记录在电子病历的自由文本中,以确保在审核期间能够被识别。