Khan Muhammad Z, Yousaf Hamza, Dahiya Dushyant S, Wani Farah, Kichloo Asim
Internal Medicine, Central Michigan University College of Medicine, Saginaw, USA.
Internal Medicine, Nishtar Medical University, Multan, PAK.
Cureus. 2020 Nov 12;12(11):e11459. doi: 10.7759/cureus.11459.
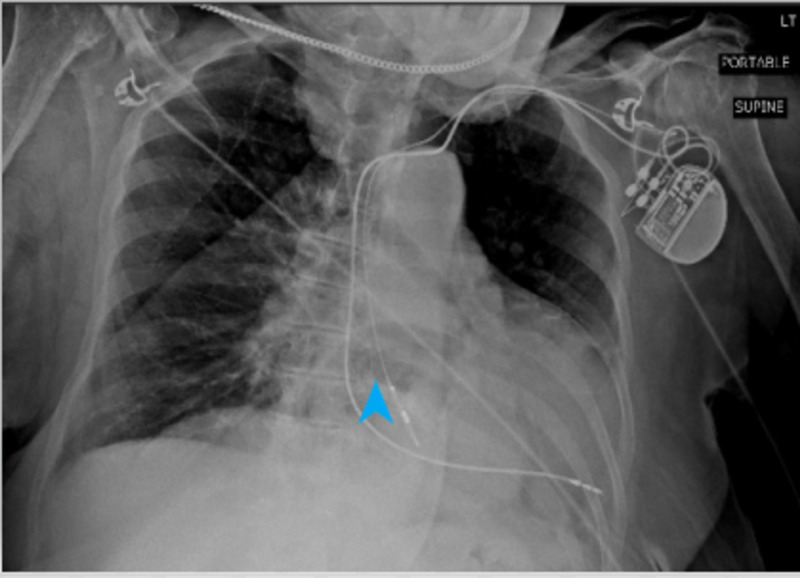
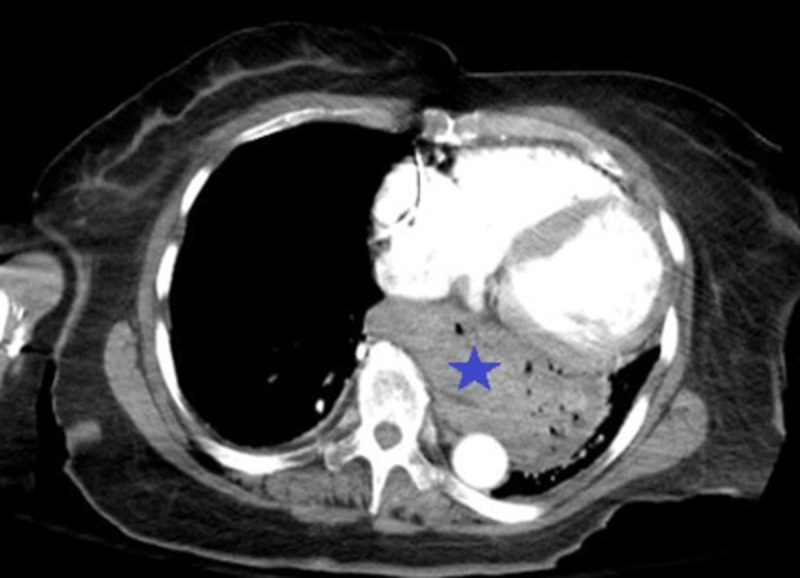
Hiatal hernia results from the translocation of intra-abdominal contents from their usual position into the thorax. They can be categorized into type I-IV which implies varying gradations of herniation. The symptomatology can range from just chest pain in the less severe types to respiratory and hemodynamic compromise resulting from strangulation in the advanced hernias. Our patient was an 81-year-old female with a past medical history of gastroesophageal reflux disease (GERD), deep venous thrombosis (DVT), hypertension, hyperlipidemia, coronary artery disease (CAD), and cerebrovascular accident (CVA), who presented to the emergency department (ED) with the chief complaint of chest pain. Assessment of the vitals in the ED revealed a temperature of 37.2 °C, respiratory rate of 18 breaths/minute with an oxygen saturation of 100% on room air, heart rate of 95 beats/min, and blood pressure reading of 132/110 mmHg. Due to significant concern of a possible coronary pathology leading to chest pain, the patient was given 325 mg of aspirin and one tablet of sublingual nitroglycerin. Her electrocardiogram (EKG) was unremarkable but the chest X-ray revealed a large retrocardiac hernia. The finding was corroborated after a review of the computerized tomography (CT) scan performed at the outlying facility. She was treated with omeprazole, a gastroenterologist was consulted, and an esophagogastroduodenoscopy (EGD) performed which revealed significant erosions in the distal esophagus and gastric antrum. She was deemed a high-risk surgical candidate for any intervention and thus managed conservatively with proton pump inhibitor (PPI) therapy. The case highlights the pertinent facts about hiatal hernia. Although the diagnosis of chest pain with the aforementioned comorbidities could be skewed towards coronary pathology, keeping a wide differential is important so that the right diagnosis can be made in a timely fashion and complications avoided.
食管裂孔疝是由于腹腔内容物从其正常位置移位至胸腔所致。它们可分为I - IV型,这意味着不同程度的疝出。症状从较轻类型的单纯胸痛到晚期疝绞窄导致的呼吸和血流动力学损害不等。我们的患者是一位81岁女性,既往有胃食管反流病(GERD)、深静脉血栓形成(DVT)、高血压、高脂血症、冠状动脉疾病(CAD)和脑血管意外(CVA)病史,因胸痛为主诉就诊于急诊科(ED)。在急诊科对生命体征的评估显示体温为37.2℃,呼吸频率为18次/分钟,在室内空气中氧饱和度为100%,心率为95次/分钟,血压读数为132/110 mmHg。由于高度怀疑可能是冠状动脉病变导致胸痛,给予患者325 mg阿司匹林和一片舌下硝酸甘油。她的心电图(EKG)无异常,但胸部X线显示巨大的心后区疝。在查阅了在外院进行的计算机断层扫描(CT)扫描结果后,这一发现得到了证实。给予她奥美拉唑治疗,咨询了胃肠病学家,并进行了食管胃十二指肠镜检查(EGD),结果显示食管远端和胃窦有明显糜烂。她被认为是任何干预措施的高风险手术候选人,因此采用质子泵抑制剂(PPI)治疗进行保守处理。该病例突出了关于食管裂孔疝的相关事实。尽管对于伴有上述合并症的胸痛诊断可能偏向于冠状动脉病变,但保持广泛的鉴别诊断很重要,以便能及时做出正确诊断并避免并发症。