Department of Rheumatology, Erasmus University Medical Center, Rotterdam, The Netherlands.
Department of Rheumatology, Leiden University Medical Center, Leiden, The Netherlands.
Rheumatology (Oxford). 2021 Aug 2;60(8):3872-3878. doi: 10.1093/rheumatology/keaa774.
According to guidelines, clinical arthritis is mandatory for diagnosing RA. However, in the absence of clinical synovitis, imaging-detected subclinical synovitis is increasingly used instead and is considered as a starting point for DMARD therapy. To search for evidence we studied the natural course of arthralgia patients with subclinical synovitis from three longitudinal cohorts and determined the frequencies of non-progression to clinically apparent inflammatory arthritis (IA) (i.e. 'false positives').
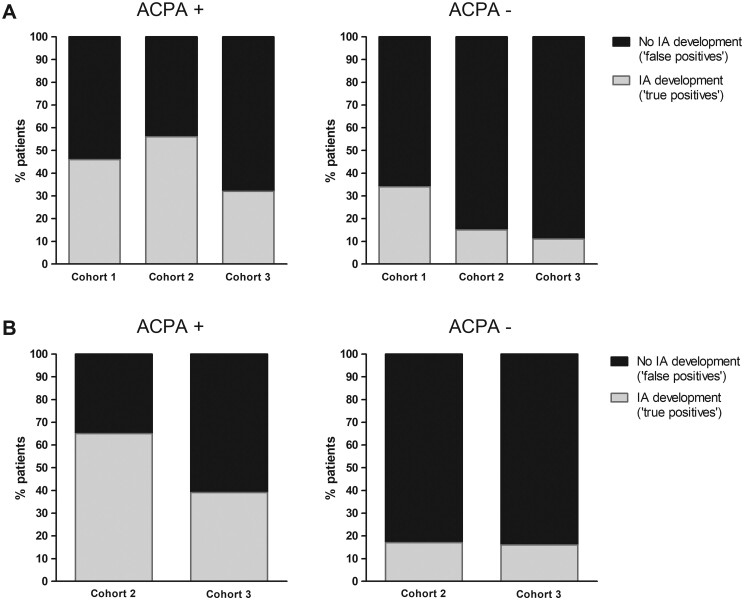
Subclinical synovitis in the hands or feet of arthralgia patients was visualized with US (two cohorts; definition: greyscale ≥2 and/or power Doppler ≥1) or MRI (one cohort; definition: synovitis score ≥1 by two readers). Patients were followed for 1 year on for IA development; two cohorts also had 3 year data. Analyses were stratified for ACPA.
Subclinical synovitis at presentation was present in 36%, 41% and 31% in the three cohorts. Of the ACPA-positive arthralgia patients with subclinical synovitis, 54%, 44% and 68%, respectively, did not develop IA. These percentages were even higher in the ACPA-negative arthralgia patients: 66%, 85% and 89%, respectively. Similar results were seen after 3 years of follow-up.
Replacing clinical arthritis with subclinical synovitis to identify RA introduces a high false-positive rate (44-89%). These data suggest an overestimation regarding the value of ACPA positivity in combination with the presence of subclinical synovitis in patients with arthralgia, which harbours the risk of overtreatment if DMARDs are initiated in the absence of clinical arthritis.
根据指南,临床关节炎是诊断 RA 的必要条件。然而,在没有临床滑膜炎的情况下,越来越多地使用影像学检测到的亚临床滑膜炎作为替代,并被认为是 DMARD 治疗的起点。为了寻找证据,我们研究了来自三个纵向队列的亚临床滑膜炎关节痛患者的自然病程,并确定了从不进展为临床明显炎症性关节炎(IA)(即“假阳性”)的频率。
使用超声(两个队列;定义:灰阶≥2 和/或能量多普勒≥1)或 MRI(一个队列;定义:两位读者的滑膜炎评分≥1)可视化关节痛患者手部或足部的亚临床滑膜炎。对患者进行 1 年的 IA 发展随访;两个队列也有 3 年的数据。分析按 ACPA 分层。
三个队列中,亚临床滑膜炎在发病时分别为 36%、41%和 31%。在亚临床滑膜炎的 ACPA 阳性关节痛患者中,分别有 54%、44%和 68%未发展为 IA。在 ACPA 阴性关节痛患者中,这一比例更高:分别为 66%、85%和 89%。在 3 年的随访后也观察到了类似的结果。
用亚临床滑膜炎替代临床关节炎来识别 RA 会导致高的假阳性率(44-89%)。这些数据表明,在关节炎患者中,将 ACPA 阳性与亚临床滑膜炎结合起来的价值被高估了,如果在没有临床关节炎的情况下开始使用 DMARD,就存在过度治疗的风险。