Leeds Institute of Rheumatic and Musculoskeletal Medicine, University of Leeds.
National Institute for Health Research, Leeds Biomedical Research Centre, Leeds Teaching Hospitals NHS Trust, Leeds, UK.
Rheumatology (Oxford). 2022 Aug 3;61(8):3192-3200. doi: 10.1093/rheumatology/keab862.
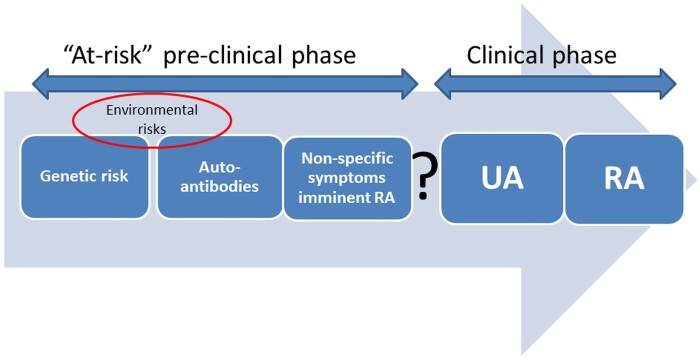
To investigate whether anti-CCP2-positive at-risk individuals with musculoskeletal (MSK) symptoms but without clinical synovitis (CCP2+ at-risk) develop US subclinical synovitis before inflammatory arthritis and if US subclinical synovitis can be predicted.
First, US scans of CCP2+ at-risk individuals who developed inflammatory arthritis ('progressors') were reviewed for subclinical synovitis prior to inflammatory arthritis development. Patients in whom the pre-progression US scan was negative but the scan was conducted >6 months before progression were excluded. Subsequently, regression analyses were performed to identify predictors of US synovitis in CCP2+ at-risk individuals without baseline US abnormalities who had one or more longitudinal US scan and a complete dataset.
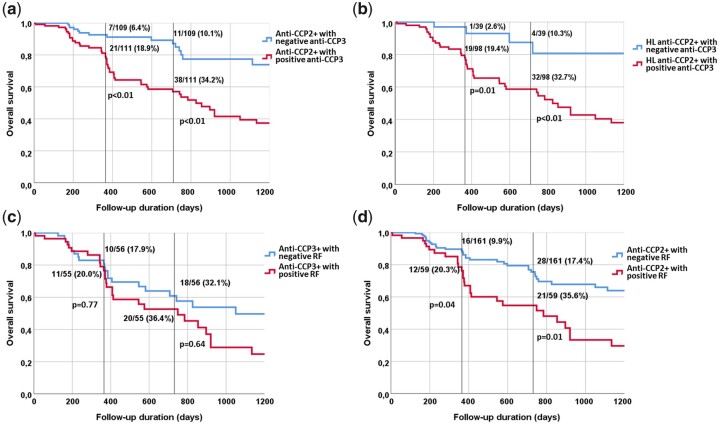
US subclinical synovitis was detected in one or more scan in 75 of 97 progressors (77.3%) {median time to inflammatory arthritis development from first evidence of US synovitis 26.5 weeks [interquartile range (IQR) 7-60]}, in whom one or more scan was available, excluding those with a negative scan >6 months from inflammatory arthritis development (n = 38). In 220 CCP2+ at-risk individuals with normal baseline US scans, who had one or more longitudinal US scan and a complete dataset, US synovitis was detected in 69/220 (31.4%) [median time to first developing US synovitis 56.4 weeks (IQR 33.0-112.0)]. In the multivariable analysis, only anti-CCP3 antibodies were predictive for the development of US synovitis [odds ratio 4.75 (95% CI 1.97, 11.46); P < 0.01].
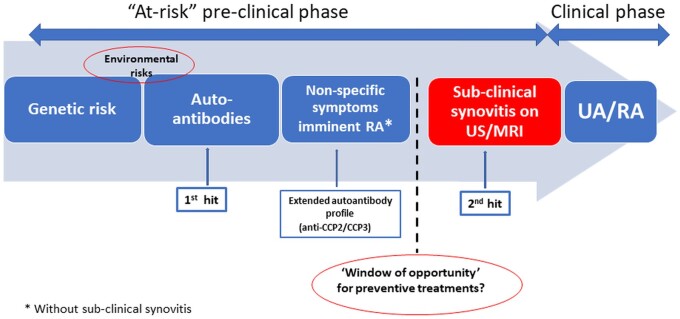
In anti-CCP2+ at-risk individuals, a stage of subclinical synovitis usually precedes the development of inflammatory arthritis. Anti-CCP2+/CCP3+ individuals without clinical or US subclinical synovitis may represent the optimal window of opportunity for intervention to prevent joint disease.
探讨是否存在抗环瓜氨酸肽 2(抗 CCP2)阳性、有肌肉骨骼(MSK)症状但无临床滑膜炎(抗 CCP2 阳性、有风险)的个体在出现炎症性关节炎之前会发生超声下亚临床滑膜炎,以及超声下亚临床滑膜炎是否可预测。
首先,回顾分析了发生炎症性关节炎(“进展者”)的抗 CCP2 阳性、有风险个体的超声检查,以评估炎症性关节炎发病前的亚临床滑膜炎情况。排除了在进展前的超声检查为阴性但检查时间距进展时间>6 个月的患者。随后,对无基线超声异常且有 1 次或多次纵向超声检查和完整数据集的抗 CCP2 阳性、无风险个体进行回归分析,以确定超声滑膜炎的预测因素。
在有一个或多个扫描的 75 名进展者(77.3%){从首次超声滑膜炎证据到炎症性关节炎发病的中位时间为 26.5 周(四分位距(IQR)7-60])中发现了超声下亚临床滑膜炎,其中一个或多个扫描可用,排除了在炎症性关节炎发病前 6 个月以上进行了阴性扫描的患者(n=38)。在 220 名基线超声检查正常、有 1 次或多次纵向超声检查和完整数据集的抗 CCP2 阳性、有风险个体中,69/220(31.4%)[从首次出现超声滑膜炎的中位时间为 56.4 周(IQR 33.0-112.0)]发现了超声滑膜炎。多变量分析显示,只有抗 CCP3 抗体是预测超声滑膜炎发展的因素[比值比(OR)4.75(95%置信区间(CI)1.97,11.46);P<0.01]。
在抗 CCP2 阳性、有风险个体中,亚临床滑膜炎通常先于炎症性关节炎发生。无临床或超声下亚临床滑膜炎的抗 CCP2/CCP3 阳性个体可能代表了预防关节疾病的最佳干预机会窗口。