Department of Internal Medicine, Seoul National University Hospital, Seoul, Korea.
Department of Internal Medicine, Seoul National University College of Medicine, Seoul, Korea.
PLoS One. 2020 Dec 17;15(12):e0244156. doi: 10.1371/journal.pone.0244156. eCollection 2020.
The estimated glomerular filtration rate (eGFR), commonly estimated using the serum creatinine value, often fluctuates throughout the serial measurement. The clinical significance of GFR variation among the general population with normal renal function has not yet been demonstrated. Thus, we explored the impact of GFR variability on adverse clinical outcomes.
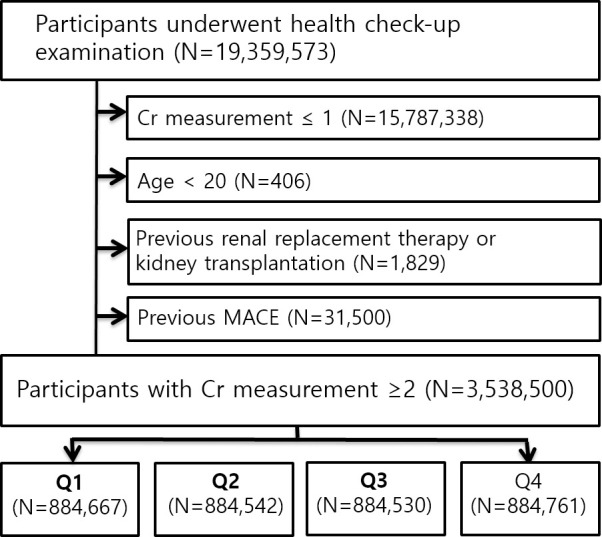
A nationwide retrospective cohort study using the Korean National Health Insurance System database was performed. National health screening examinees who underwent creatinine measurement ≥3 times between 2012 and 2016 were considered. Those with eGFR under 60 mL/min/m2 were excluded. The fluctuation of eGFR was represented with variability independent of the mean (VIM) index; which was calculated by the standard deviation divided by the exponent of the regression coefficient of the mean. Then, the risks of myocardial infarction (MI), stroke and death were assessed according to the quartiles of the VIM.
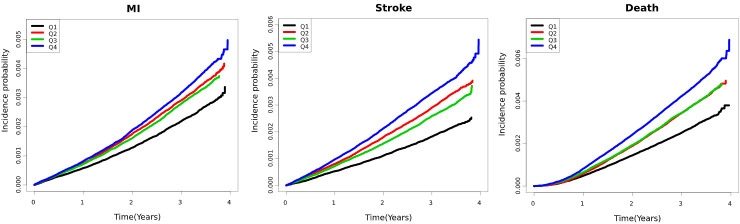
Of total 3,538,500 participants, 0.29% of myocardial infarction (MI), 0.14% of stroke, 0.36% of deaths were observed during the median follow up of 3.27 years. Participants with the highest VIM index, which represents the highest eGFR variability, were significantly associated with an increased risk of MI (hazard ratio [HR]; 1.10, 95% confidence interval [95% CI]; 1.04-1.16), stroke (HR: 1.16; 95% CI 1.09-1.23), and death (HR: 1.18; 95% CI 1.12-1.24). The elevated risk of adverse events was consistent after the multivariate adjustment with potential confounding factors, except the risk of MI (HR 1.06; 95% 1.00-1.06).
Increased eGFR variability exhibited an association with major clinical outcomes, indicating that monitoring eGFR variability might be a useful parameter for predicting the adverse outcomes.
估算肾小球滤过率(eGFR)通常使用血清肌酐值估算,但在连续测量过程中常常波动。具有正常肾功能的普通人群中 GFR 变化的临床意义尚未得到证实。因此,我们探讨了 GFR 变异性对不良临床结局的影响。
使用韩国国家健康保险系统数据库进行全国性回顾性队列研究。研究对象为 2012 年至 2016 年间至少进行过 3 次肌酐测量的国家健康筛查受检者。排除 eGFR 低于 60 mL/min/m2 的患者。eGFR 的波动用均值独立变异(VIM)指数表示;通过均值回归系数的标准差除以指数来计算。然后,根据 VIM 的四分位数评估心肌梗死(MI)、中风和死亡的风险。
在总共 3538500 名参与者中,中位随访 3.27 年期间,观察到 0.29%的 MI、0.14%的中风和 0.36%的死亡。VIM 指数最高(代表 GFR 变异性最高)的患者发生 MI(风险比[HR]:1.10,95%置信区间[95%CI]:1.04-1.16)、中风(HR:1.16;95%CI 1.09-1.23)和死亡(HR:1.18;95%CI 1.12-1.24)的风险显著增加。在调整了潜在混杂因素后,除 MI 风险(HR 1.06;95%CI 1.00-1.06)外,不良事件的风险仍保持升高。
增加的 eGFR 变异性与主要临床结局相关,表明监测 eGFR 变异性可能是预测不良结局的有用参数。