Division of Thoracic Surgery, Department of Surgery, Taipei Veterans General Hospital, Taipei, Taiwan.
Institute of Clinical Medicine, School of Medicine, National Yang-Ming University, Taipei, Taiwan.
Interact Cardiovasc Thorac Surg. 2021 Apr 19;32(4):537-545. doi: 10.1093/icvts/ivaa297.
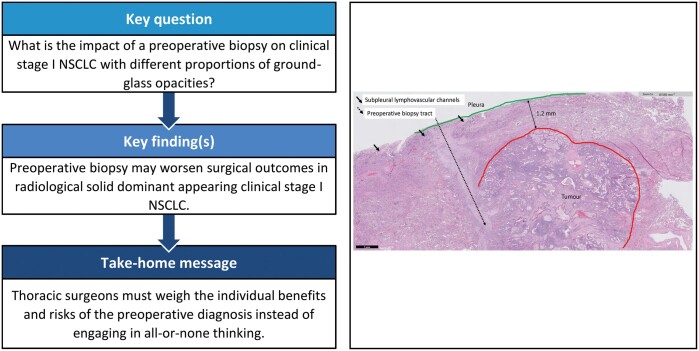
The present study aimed to clarify the association between preoperative biopsy and surgical outcomes in clinical stage I non-small-cell lung cancer (NSCLC) with different proportions of ground-glass opacity (GGO).
Data on patients who underwent pulmonary resection for NSCLC from 2006 to 2016 were drawn from a prospective registered database and analysed retrospectively. Patient characteristics collected included tumour size, location and staging, surgical approach, consolidation-tumour ratio, histopathology and the presence or absence of preoperative biopsy to identify the independent prognostic factors of disease-free survival (DFS) and cancer-specific survival. A 1:1 propensity score matching was conducted between the preoperative biopsy and reference groups based on their baseline characteristics measured before the decision for preoperative biopsy.
A total of 1427 patients were collected to achieve an overall 5-year DFS as 84.5% (median follow-up: 67.3 months), stratified to be 99.5% in the GGO-dominant group (n = 430) and 78.2% in the solid-dominant group (n = 997). Only 2 patients (0.5%) in the GGO-dominant group experienced tumour recurrence. For solid-dominant tumours matched with propensity scores (279 in preoperative biopsy vs 279 in reference group), the independent predictors of DFS included preoperative biopsy, sublobar resection, pathological staging and angiolymphatic invasion. Preoperative biopsy was a predictor of cancer-specific survival in univariable analysis but was not in multivariable analysis. Significant differences were also found between matched groups in those with late-delay surgery, but not in patients receiving preoperative biopsy with early-delay surgery (≤21 days).
Preoperative biopsy may worsen surgical outcomes in patients with clinical stage I, solid-dominant NSCLC.
本研究旨在明确不同磨玻璃密度(GGO)比例的临床Ⅰ期非小细胞肺癌(NSCLC)患者术前活检与手术结果之间的关系。
从前瞻性注册数据库中提取了 2006 年至 2016 年间接受 NSCLC 肺切除术的患者数据,并进行回顾性分析。收集的患者特征包括肿瘤大小、位置和分期、手术方式、实变/肿瘤比值、组织病理学以及术前活检的存在与否,以确定无病生存(DFS)和癌症特异性生存的独立预后因素。根据术前活检前的基线特征,对术前活检组和对照组进行了 1:1 的倾向评分匹配。
共收集了 1427 例患者,总体 5 年 DFS 为 84.5%(中位随访时间:67.3 个月),GGO 优势组(n=430)为 99.5%,实性优势组(n=997)为 78.2%。GGO 优势组仅 2 例(0.5%)患者发生肿瘤复发。在实性优势肿瘤中匹配倾向评分(术前活检 279 例,对照组 279 例),DFS 的独立预测因素包括术前活检、亚肺叶切除术、病理分期和血管淋巴管侵犯。术前活检在单变量分析中是癌症特异性生存的预测因素,但在多变量分析中不是。在延迟手术时间较长的匹配组中也发现了显著差异,但在接受早期延迟手术(≤21 天)的患者中没有发现差异。
术前活检可能会使临床Ⅰ期实性优势 NSCLC 患者的手术结果恶化。