Department of Emergency Medicine, University of Michigan Medical School, 2800 Plymouth Road, Ann Arbor, MI, 48109, USA; Michigan Center for Integrative Research in Critical Care, University of Michigan Medical School, 2800 Plymouth Road, Ann Arbor, MI, 48109, USA; Department of Surgery, University of Michigan Medical School, 2800 Plymouth Road, Ann Arbor, MI, 48109, USA.
Department of Emergency Medicine, University of Michigan Medical School, 2800 Plymouth Road, Ann Arbor, MI, 48109, USA; Michigan Center for Integrative Research in Critical Care, University of Michigan Medical School, 2800 Plymouth Road, Ann Arbor, MI, 48109, USA.
Resuscitation. 2021 Feb;159:28-34. doi: 10.1016/j.resuscitation.2020.12.004. Epub 2020 Dec 15.
It remains unclear whether cardiac arrest (CA) resuscitation generates aerosols that can transmit respiratory pathogens. We hypothesize that chest compression and defibrillation generate aerosols that could contain the SARS-CoV-2 virus in a swine CA model.
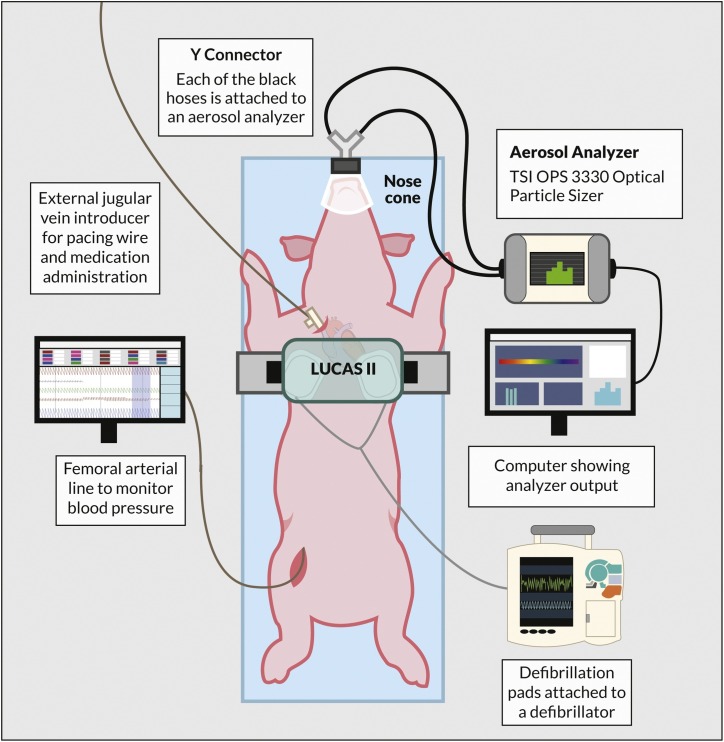
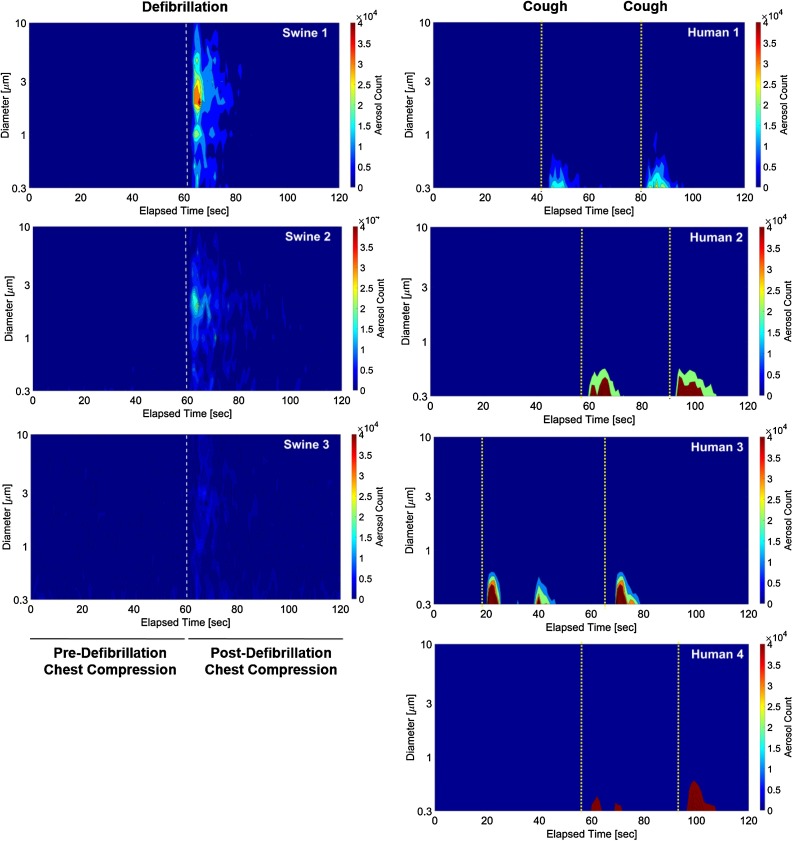
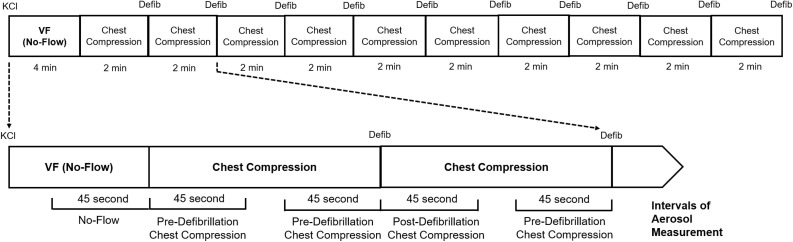
To simulate witnessed CA with bystander-initiated cardiopulmonary resuscitation, 3 female non-intubated swine underwent 4 min of ventricular fibrillation without chest compression or defibrillation (no-flow) followed by ten 2-min cycles of mechanical chest compression and defibrillation without ventilation. The diameter (0.3-10 μm) and quantity of aerosols generated during 45-s intervals of no-flow and chest compression before and after defibrillation were analyzed by a particle analyzer. Aerosols generated from the coughs of 4 healthy human subjects were also compared to aerosols generated by swine.
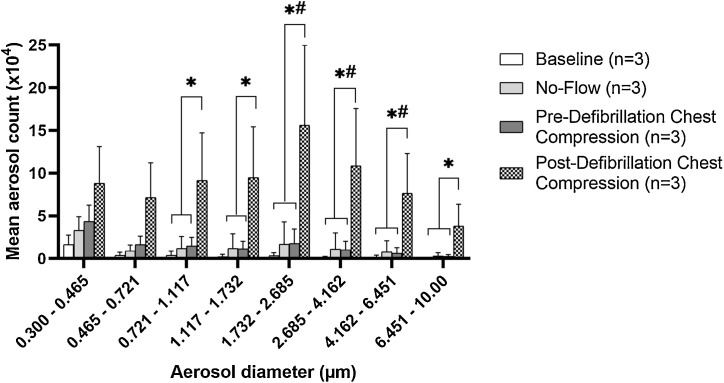
There was no significant difference between the total aerosols generated during chest compression before defibrillation compared to no-flow. In contrast, chest compression after defibrillation generated significantly more aerosols than chest compression before defibrillation or no-flow (72.4 ± 41.6 × 10 vs 12.3 ± 8.3 × 10 vs 10.5 ± 11.2 × 10; p < 0.05), with a shift in particle size toward larger aerosols. Two consecutive human coughs generated 54.7 ± 33.9 × 10 aerosols with a size distribution smaller than post-defibrillation chest compression.
Chest compressions alone did not cause significant aerosol generation in this swine model. However, increased aerosol generation was detected during chest compression immediately following defibrillation. Additional research is needed to elucidate the clinical significance and mechanisms by which aerosol generation during chest compression is modified by defibrillation.
心脏骤停(CA)复苏是否会产生可传播呼吸道病原体的气溶胶仍不清楚。我们假设胸外按压和除颤会产生含有 SARS-CoV-2 病毒的气溶胶,这在猪 CA 模型中可以得到验证。
为了模拟有旁观者启动心肺复苏的目击性 CA,3 头未经插管的雌性猪经历了 4 分钟的心室颤动,没有进行胸外按压或除颤(无血流),然后进行了 10 个 2 分钟的机械胸外按压和除颤循环,没有通气。在无血流和除颤前后的 45 秒间隔内,通过粒子分析仪分析产生的气溶胶的直径(0.3-10μm)和数量。还将 4 名健康人体咳嗽产生的气溶胶与猪产生的气溶胶进行了比较。
与无血流相比,除颤前的胸外按压过程中产生的总气溶胶量没有显著差异。相比之下,除颤后的胸外按压比除颤前的胸外按压或无血流产生的气溶胶明显更多(72.4±41.6×10 对 12.3±8.3×10 对 10.5±11.2×10;p<0.05),并且颗粒大小分布向较大的气溶胶转移。连续两次人体咳嗽产生了 54.7±33.9×10 的气溶胶,其粒径分布小于除颤后的胸外按压。
在本猪模型中,单独的胸外按压不会导致明显的气溶胶产生。然而,在除颤后立即进行胸外按压时,检测到气溶胶生成增加。需要进一步研究阐明在胸外按压过程中,除颤如何改变气溶胶生成的临床意义和机制。