Univ. Lille, CHU Lille, ULR 2694 - METRICS, Évaluation des technologies de santé et des pratiques médicales, F-59000, Lille, France.
French national out-of-hospital cardiac arrest registry, Registre électronique des Arrêts Cardiaques, Lille, France.
Scand J Trauma Resusc Emerg Med. 2020 Dec 18;28(1):119. doi: 10.1186/s13049-020-00813-x.
The COVID-19 outbreak requires a permanent adaptation of practices. Cardiopulmonary resuscitation (CPR) is also involved and we evaluated these changes in the management of out-of-hospital cardiac arrest (OHCA).
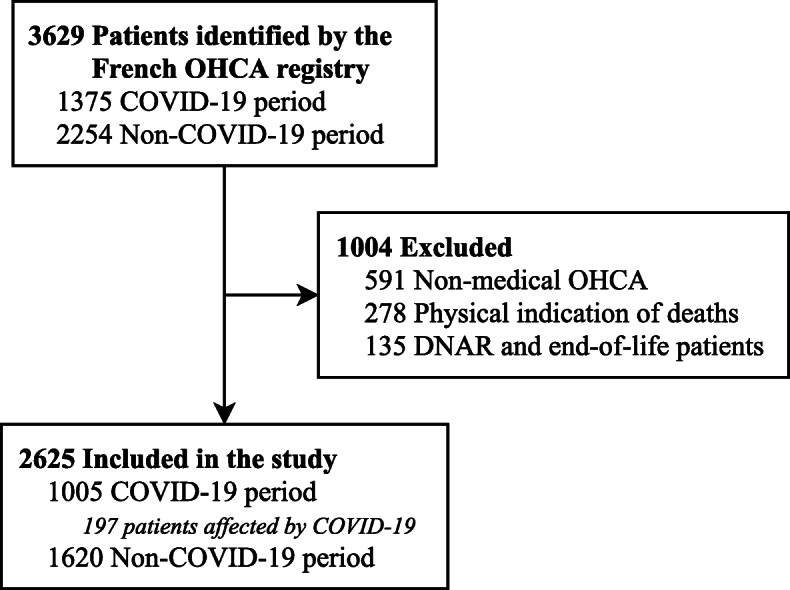
OHCA of medical origins identified from the French National Cardiac Arrest Registry between March 1st and April 31st 2020 (COVID-19 period), were analysed. Different resuscitation characteristics were compared with the same period from the previous year (non-COVID-19 period).
Overall, 1005 OHCA during the COVID-19 period and 1620 during the non-COVID-19 period were compared. During the COVID-19 period, bystanders and first aid providers initiated CPR less frequently (49.8% versus 54.9%; difference, - 5.1 percentage points [95% CI, - 9.1 to - 1.2]; and 84.3% vs. 88.7%; difference, - 4.4 percentage points [95% CI, - 7.1 to - 1.6]; respectively) as did mobile medical teams (67.3% vs. 75.0%; difference, - 7.7 percentage points [95% CI, - 11.3 to - 4.1]). First aid providers used defibrillators less often (66.0% vs. 74.1%; difference, - 8.2 percentage points [95% CI, - 11.8 to - 4.6]). Return of spontaneous circulation (ROSC) and D30 survival were lower during the COVID-19 period (19.5% vs. 25.3%; difference, - 5.8 percentage points [95% CI, - 9.0 to - 2.5]; and 2.8% vs. 6.4%; difference, - 3.6 percentage points [95% CI, - 5.2 to - 1.9]; respectively).
During the COVID-19 period, we observed a decrease in CPR initiation regardless of whether patients were suspected of SARS-CoV-2 infection or not. In the current atmosphere, it is important to communicate good resuscitation practices to avoid drastic and lasting reductions in survival rates after an OHCA.
COVID-19 疫情要求我们对实践进行永久性的调整。心肺复苏术(CPR)也受到了影响,我们评估了 COVID-19 期间院外心脏骤停(OHCA)管理中的这些变化。
从 2020 年 3 月 1 日至 4 月 31 日(COVID-19 期间)的法国国家心脏骤停登记处中分析了源于医学原因的 OHCA。将不同的复苏特征与前一年的同期(非 COVID-19 期间)进行了比较。
总体而言,比较了 COVID-19 期间的 1005 例 OHCA 和非 COVID-19 期间的 1620 例 OHCA。在 COVID-19 期间,旁观者和急救人员进行 CPR 的频率较低(49.8%对 54.9%;差异,-5.1 个百分点[95%置信区间,-9.1 至-1.2];和 84.3%对 88.7%;差异,-4.4 个百分点[95%置信区间,-7.1 至-1.6]),移动医疗团队也是如此(67.3%对 75.0%;差异,-7.7 个百分点[95%置信区间,-11.3 至-4.1])。急救人员使用除颤器的频率较低(66.0%对 74.1%;差异,-8.2 个百分点[95%置信区间,-11.8 至-4.6])。COVID-19 期间,自主循环恢复(ROSC)和 D30 生存率较低(19.5%对 25.3%;差异,-5.8 个百分点[95%置信区间,-9.0 至-2.5];和 2.8%对 6.4%;差异,-3.6 个百分点[95%置信区间,-5.2 至-1.9])。
在 COVID-19 期间,我们观察到无论患者是否疑似 SARS-CoV-2 感染,CPR 的启动率都有所下降。在当前的情况下,重要的是要传达良好的复苏实践,以避免 OHCA 后生存率的急剧和持久下降。