Bates Jason H T, Gaver Donald P, Habashi Nader M, Nieman Gary F
Department of Medicine, University of Vermont, Burlington, VT.
Department of Biomedical Engineering, Tulane University, New Orleans, LA.
Crit Care Explor. 2020 Dec 16;2(12):e0299. doi: 10.1097/CCE.0000000000000299. eCollection 2020 Dec.
Elucidate how the degree of ventilator-induced lung injury due to atelectrauma that is produced in the injured lung during mechanical ventilation is determined by both the timing and magnitude of the airway pressure profile.
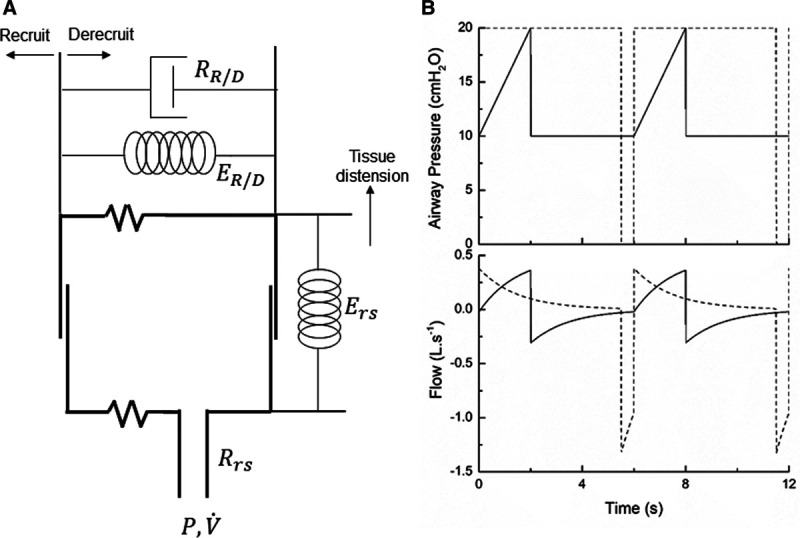
A computational model of the injured lung provides a platform for exploring how mechanical ventilation parameters potentially modulate atelectrauma and volutrauma. This model incorporates the time dependence of lung recruitment and derecruitment, and the time-constant of lung emptying during expiration as determined by overall compliance and resistance of the respiratory system.
Computational model.
Simulated scenarios representing patients with both normal and acutely injured lungs.
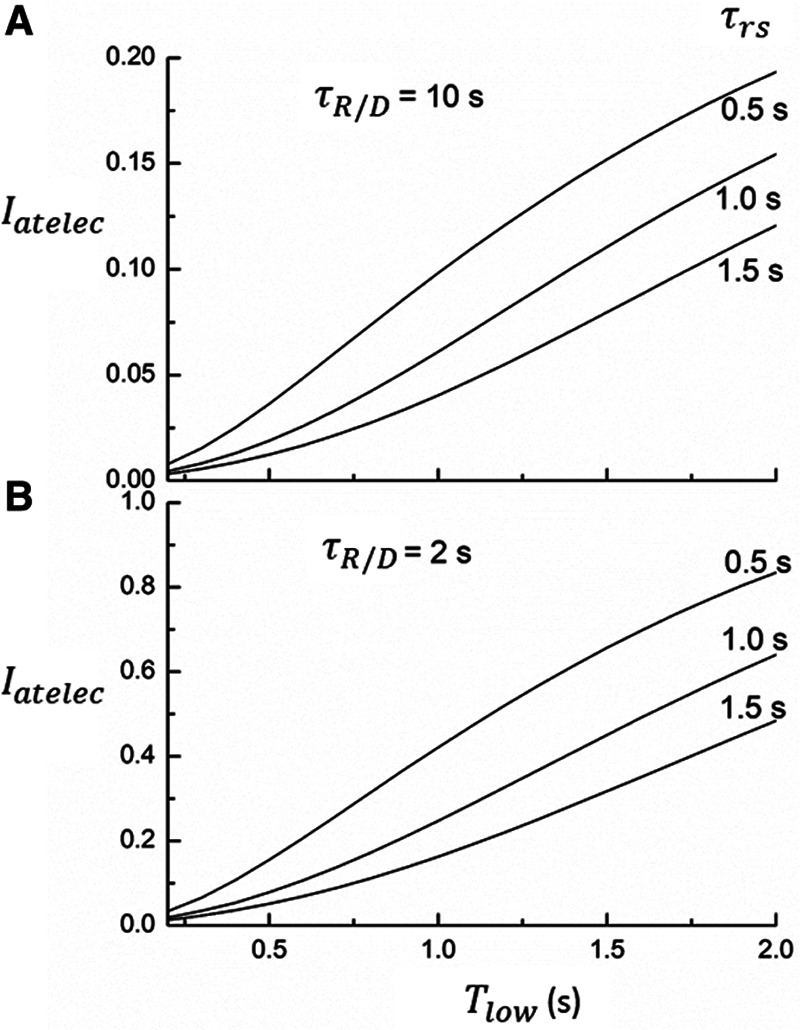
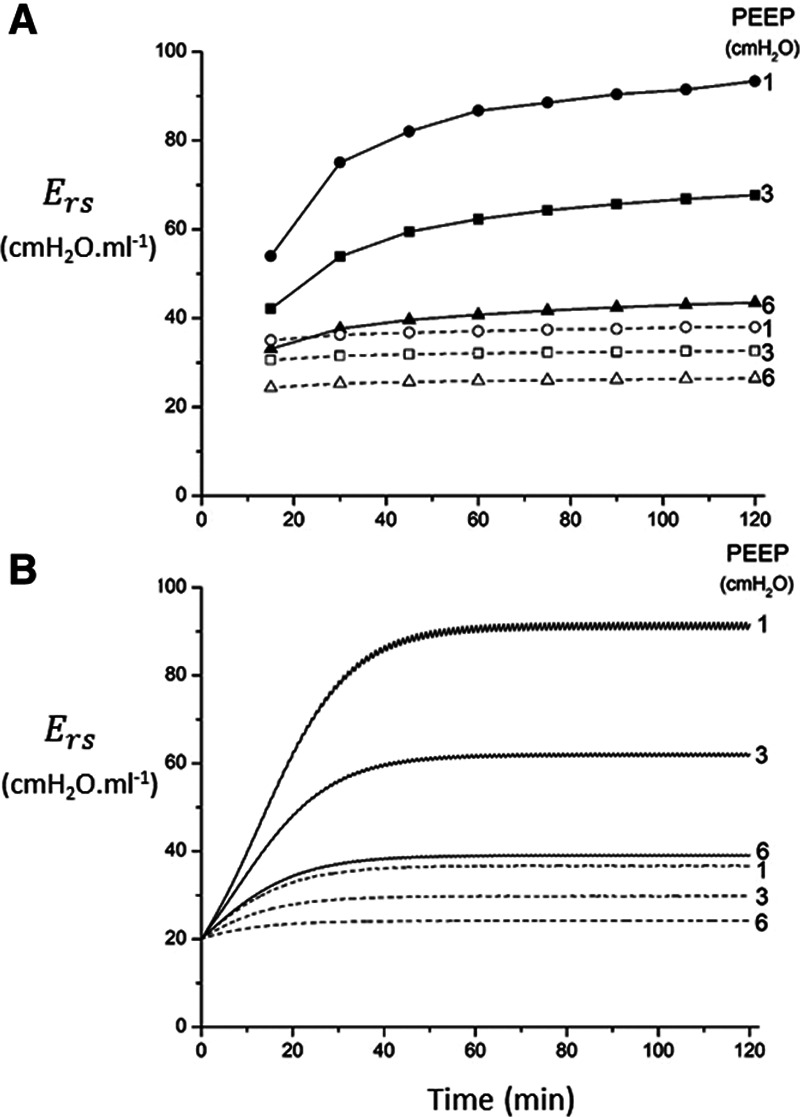
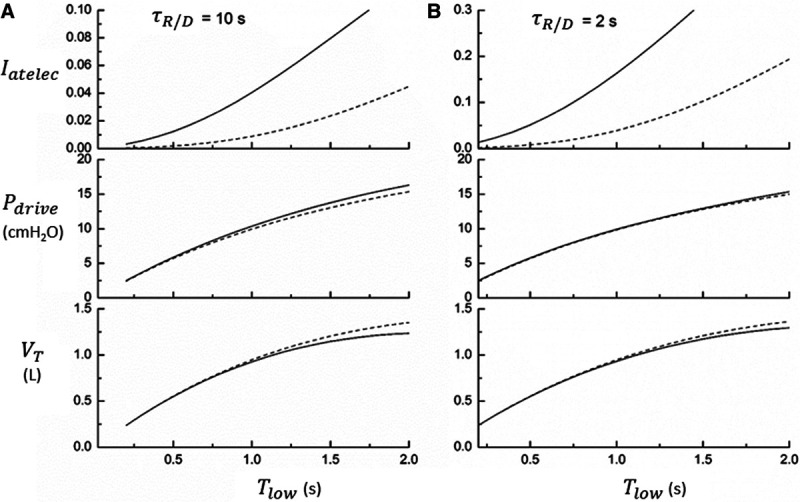
Protective low-tidal volume ventilation (Low-Vt) of the simulated injured lung avoided atelectrauma through the elevation of positive end-expiratory pressure while maintaining fixed tidal volume and driving pressure. In contrast, airway pressure release ventilation avoided atelectrauma by incorporating a very brief expiratory duration () that both prevents enough time for derecruitment and limits the minimum alveolar pressure prior to inspiration. Model simulations demonstrated that has an effective threshold value below which airway pressure release ventilation is safe from atelectrauma while maintaining a tidal volume and driving pressure comparable with those of Low-Vt. This threshold is strongly influenced by the time-constant of lung-emptying.
Low-Vt and airway pressure release ventilation represent markedly different strategies for the avoidance of ventilator-induced lung injury, primarily involving the manipulation of positive end-expiratory pressure and , respectively. can be based on exhalation flow values, which may provide a patient-specific approach to protective ventilation.
阐明在机械通气期间,因肺损伤时产生的肺不张伤所导致的呼吸机相关性肺损伤程度是如何由气道压力曲线的时机和幅度共同决定的。
受损肺的计算模型为探索机械通气参数如何潜在地调节肺不张伤和容积伤提供了一个平台。该模型纳入了肺复张和肺萎陷的时间依赖性,以及由呼吸系统的总体顺应性和阻力所决定的呼气期间肺排空的时间常数。
计算模型。
代表正常肺和急性损伤肺患者的模拟场景。
模拟受损肺的保护性小潮气量通气(低Vt)通过提高呼气末正压来避免肺不张伤,同时保持固定的潮气量和驱动压力。相比之下,气道压力释放通气通过纳入非常短暂的呼气持续时间()来避免肺不张伤,这既能防止有足够时间发生肺萎陷,又能限制吸气前的最低肺泡压力。模型模拟表明,有一个有效阈值,低于该阈值时,气道压力释放通气在保持与低Vt相当的潮气量和驱动压力的同时,可避免肺不张伤。这个阈值受肺排空时间常数的强烈影响。
低Vt和气道压力释放通气代表了截然不同的避免呼吸机相关性肺损伤的策略,主要分别涉及对呼气末正压和的操控。可基于呼气流量值来确定,这可能为保护性通气提供一种针对患者的方法。