School of Dental Sciences, Newcastle University, United Kingdom; Newcastle upon Tyne Hospitals NHS Foundation Trust, Newcastle Upon Tyne, United Kingdom.
School of Dental Sciences, Newcastle University, United Kingdom; Newcastle upon Tyne Hospitals NHS Foundation Trust, Newcastle Upon Tyne, United Kingdom.
J Dent. 2021 Feb;105:103565. doi: 10.1016/j.jdent.2020.103565. Epub 2021 Jan 6.
Identify splatter/aerosol distribution from dental procedures in an open plan clinic and explore aerosol settling time after dental procedures.
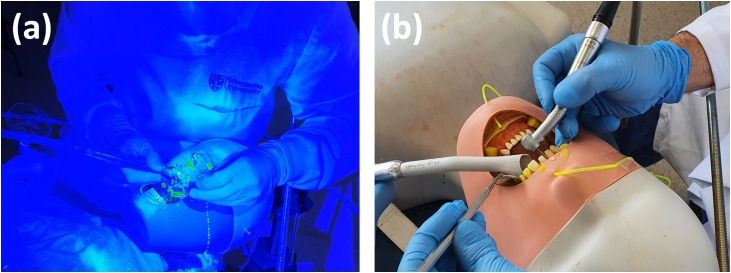
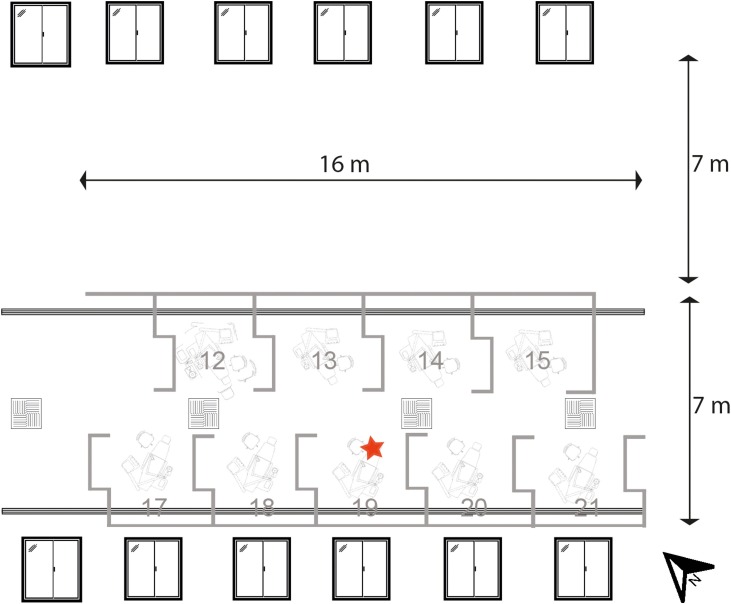
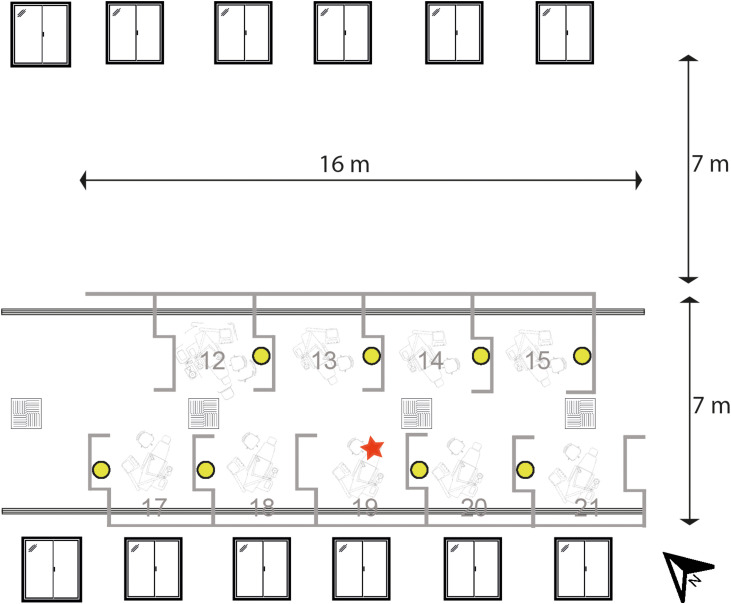
In two experimental designs using simulated dental procedures on a mannequin, fluorescein dye was introduced: (1) into the irrigation system of an air-turbine handpiece; (2) into the mannequin's mouth. Filter papers were placed in an open plan clinic to collect fluorescein. An 8-metre diameter rig was used to investigate aerosol settling time. Analysis was by fluorescence photography and spectrofluorometry.
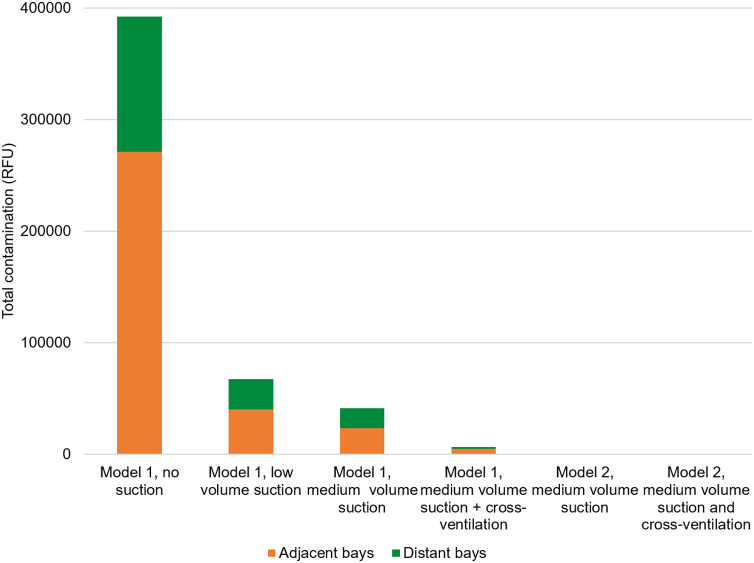
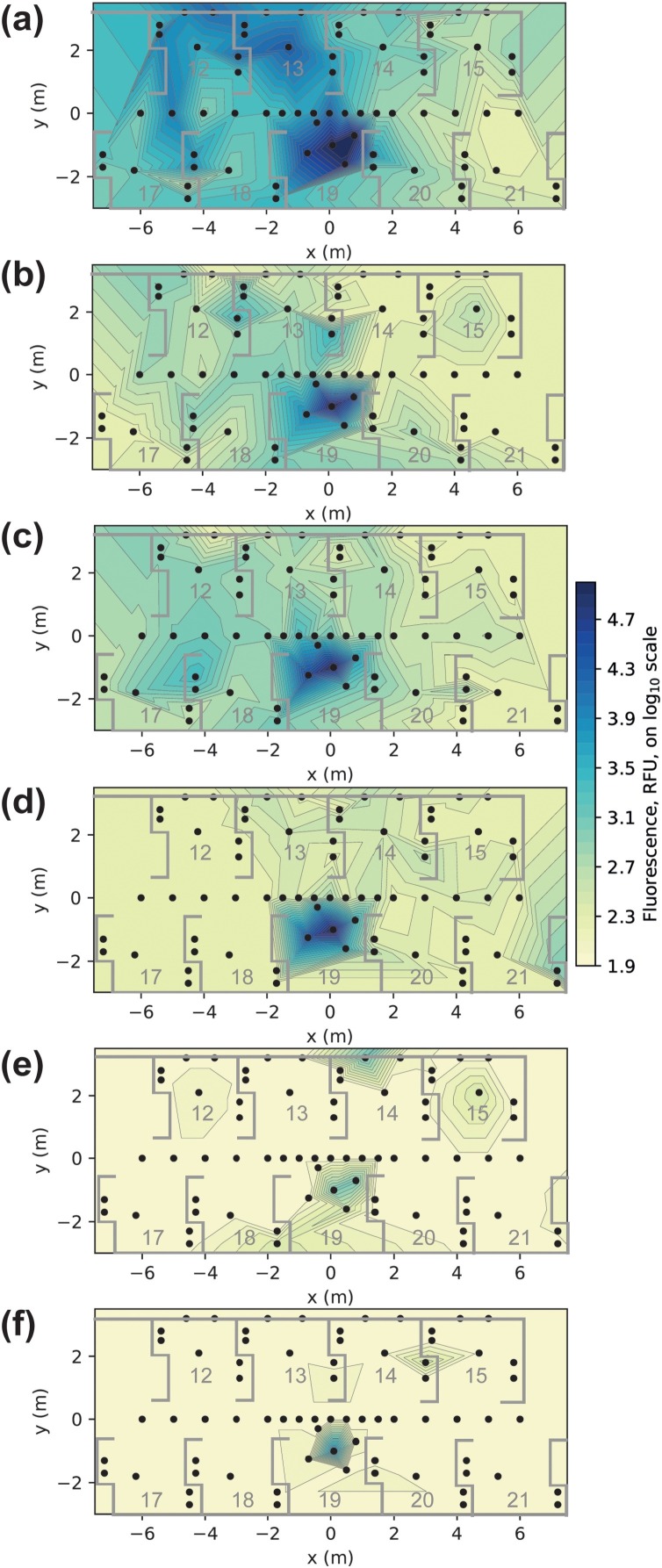
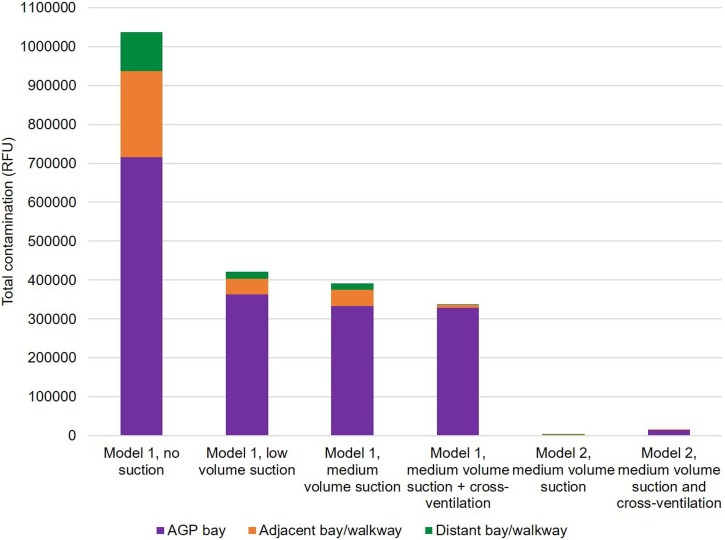
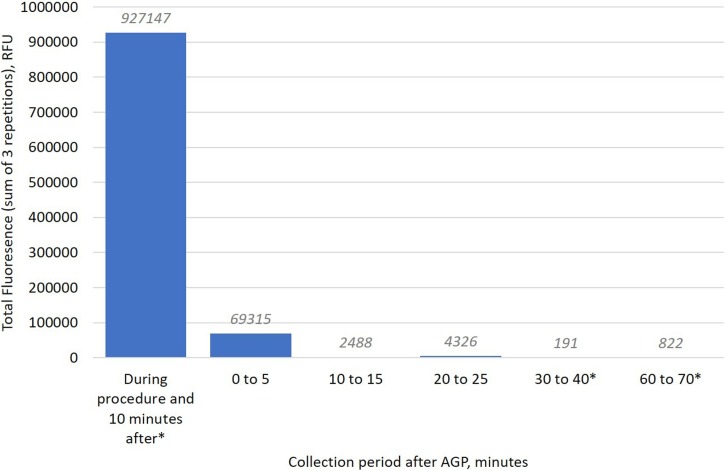
Contamination distribution varied across the clinic depending on conditions. Unmitigated procedures have the potential to deposit contamination at large distances. Medium volume dental suction (159 L/min air) reduced contamination in the procedural bay by 53%, and in other areas by 81-83%. Low volume suction (40 L/min air) was similar. Cross-ventilation reduced contamination in adjacent and distant areas by 80-89%. In the most realistic model (fluorescein in mouth, medium volume suction), samples in distant bays (≥5 m head-to-head chair distance) gave very low or zero readings (< 0.0016% of the fluorescein used during the procedure). Almost all (99.99%) of the splatter detected was retained within the procedural bay/walkway. After 10 min, very little additional aerosol settled.
Cross-infection risk from dental procedures in an open plan clinic appears small when bays are ≥ 5 m apart. Dilution effects from instrument water spray were observed, and dental suction is of benefit. Most settled aerosol is detected within 10 min indicating environmental cleaning may be appropriate after this.
Aerosols produced by dental procedures have the potential to contaminate distant sites and the majority of settled aerosol is detectable after 10 min. Dental suction and ventilation have a substantial beneficial effect. Contamination is likely to be minimal in open plan clinics at distances of 5 m or more.
识别开放式诊室牙科操作中的飞沫/气溶胶分布,并探讨牙科操作后气溶胶沉降时间。
在使用仿头模进行模拟牙科操作的两项实验设计中,引入了荧光染料:(1)在高速手机的冲洗系统中;(2)在头模口腔内。在开放式诊室中放置滤纸条以收集荧光染料。使用 8 米直径的装置来研究气溶胶沉降时间。分析方法为荧光摄影和荧光分光光度法。
根据条件的不同,污染分布在整个诊室中各不相同。未采取缓解措施的操作有在远距离沉积污染物的潜力。中流量牙科抽吸(159 L/min 空气)使操作舱内的污染减少了 53%,其他区域减少了 81-83%。低流量抽吸(40 L/min 空气)效果类似。交叉通风使相邻和远处区域的污染减少了 80-89%。在最现实的模型(口腔内荧光染料,中流量抽吸)中,远处隔室(≥5 米对头椅距离)的样本读数非常低或为零(< 操作过程中使用的荧光染料的 0.0016%)。检测到的几乎所有(99.99%)飞沫都被保留在操作舱/通道内。10 分钟后,沉降的气溶胶几乎没有增加。
当隔室之间的距离≥5 米时,开放式诊室牙科操作的交叉感染风险似乎很小。观察到仪器水喷雾的稀释效应,并且牙科抽吸具有有益效果。大多数沉降的气溶胶在 10 分钟内被检测到,这表明环境清洁可能在 10 分钟后进行。
牙科操作产生的气溶胶有可能污染远处的场所,而大多数沉降的气溶胶在 10 分钟后可被检测到。牙科抽吸和通风具有显著的有益效果。在距离 5 米或更远的开放式诊室中,污染可能很少。