Ma Bing-Qiang, Chen Shi-Yong, Jiang Ze-Bin, Wu Biao, He Yu, Wang Xin-Xin, Li Yuan, Gao Peng, Yang Xiao-Jun
Department of General Surgery, Gansu Provincial Hospital, Lanzhou 730000, Gansu Province, China.
School of Clinical Medicine, Ningxia Medical University, Yinchuan 750000, Ningxia Hui Autonomous Region, China.
World J Gastroenterol. 2020 Dec 14;26(46):7405-7415. doi: 10.3748/wjg.v26.i46.7405.
Most cholangiocarcinoma patients with malignant obstructive jaundice (MOJ) have varying degrees of malnutrition and immunodeficiency preoperatively. Therefore, perioperative nutritional support has important clinical significance in the treatment of cholangiocarcinoma.
To investigate the effects of postoperative early enteral nutrition (EEN) on immunity function and clinical outcomes of cholangiocarcinoma patients with MOJ.
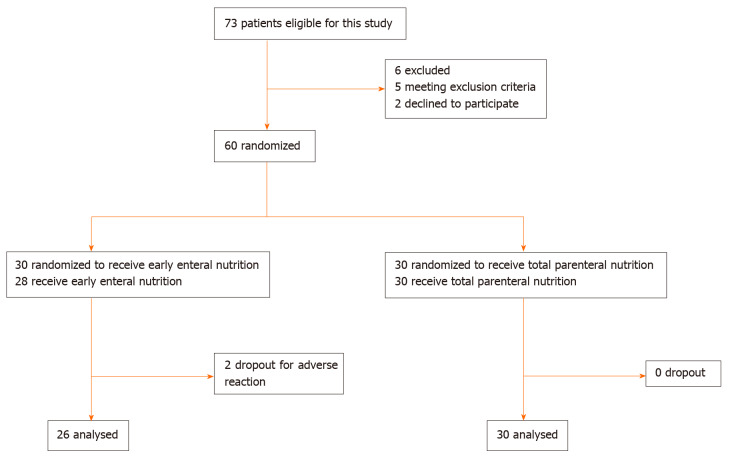
This prospective clinical study included 60 cholangiocarcinoma patients with MOJ who underwent surgery. The patients were randomly divided into an experimental group and a control group according to the nutrition support modes. The control group received postoperative total parenteral nutrition (TPN), whereas the experimental group received postoperative EEN and parenteral nutrition (PN; EEN + PN). The clinical outcomes, postoperative immune function, incidences of surgical site infection and bile leakage, intestinal function recovery time, average hospitalization days, and hospitalization expenses of the two groups were assessed on postoperative days (PODs) 1, 3, and 7.
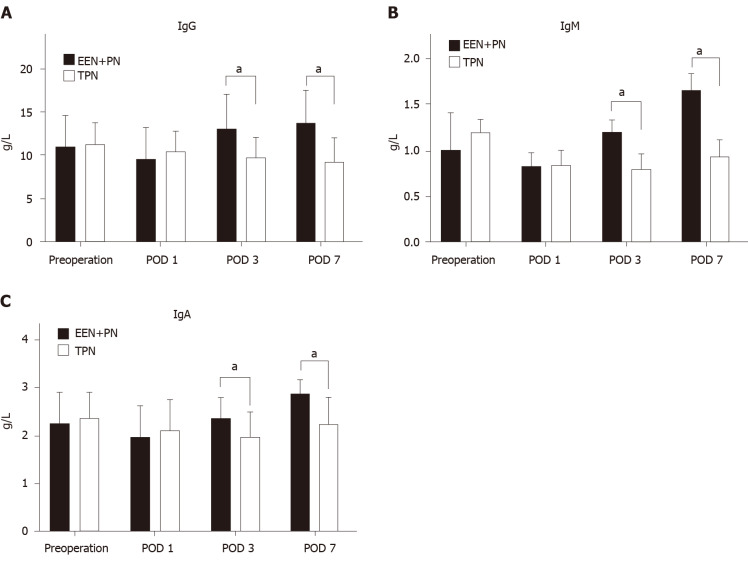
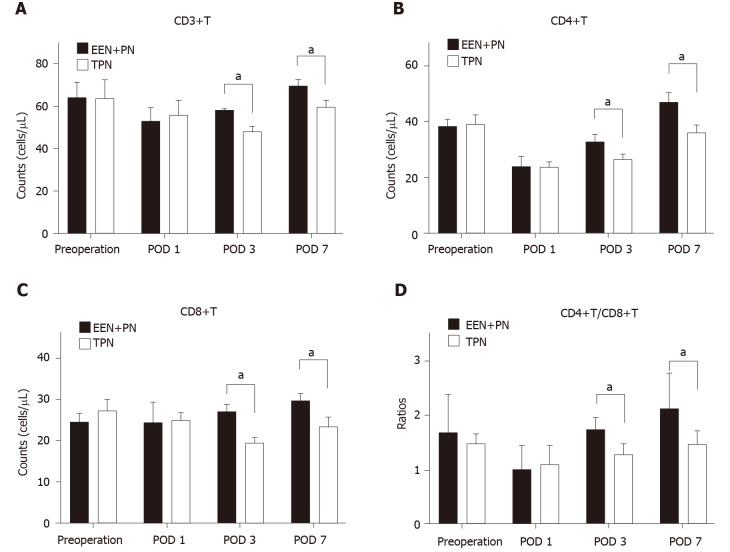
The CD3+T, CD4+T, CD8+T, and CD4+T/CD8+T cell count and the immunoglobulin (Ig) G, IgM, and IgA levels in the EEN + PN group were significantly higher than those in the TPN group on PODs 3 and 7 ( < 0.05), whereas no significant differences in the CD3+T, CD4+T, CD8+T, and CD4+T/CD8+T cell counts and IgG, IgM, and IgA levels before operation and on POD 1 were found between the two groups ( > 0.05). The intestinal function recovery time and postoperative hospital stay were shorter ( < 0.001 for both) in the EEN + PN group than in the TPN group. The hospitalization expenses of the EEN + PN group were lower than those of the TPN group ( < 0.001). However, the incidence of abdominal distension was higher than in the EEN + PN group than in the TPN group ( < 0.05). The incidence rates of biliary leakage and surgical site infection were not significantly different between the two groups ( > 0.05).
A postoperative EEN program could reduce the incidence of postoperative complications and improve the clinical outcomes and immune functions of cholangiocarcinoma patients with MOJ and is thus beneficial to patient recovery.
大多数恶性梗阻性黄疸(MOJ)胆管癌患者术前存在不同程度的营养不良和免疫功能低下。因此,围手术期营养支持在胆管癌治疗中具有重要的临床意义。
探讨术后早期肠内营养(EEN)对MOJ胆管癌患者免疫功能和临床结局的影响。
这项前瞻性临床研究纳入了60例行手术治疗的MOJ胆管癌患者。根据营养支持方式将患者随机分为实验组和对照组。对照组接受术后全肠外营养(TPN),而实验组接受术后EEN联合肠外营养(PN;EEN + PN)。在术后第1、3和7天评估两组的临床结局、术后免疫功能、手术部位感染和胆漏发生率、肠功能恢复时间、平均住院天数和住院费用。
在术后第3天和第7天,EEN + PN组的CD3 + T、CD4 + T、CD8 + T和CD4 + T/CD8 + T细胞计数以及免疫球蛋白(Ig)G、IgM和IgA水平显著高于TPN组(P < 0.05),而两组术前和术后第1天的CD3 + T、CD4 + T、CD8 + T和CD4 + T/CD8 + T细胞计数以及IgG、IgM和IgA水平无显著差异(P > 0.05)。EEN + PN组的肠功能恢复时间和术后住院时间均短于TPN组(两者均P < 0.001)。EEN + PN组的住院费用低于TPN组(P < 0.001)。然而,EEN + PN组腹胀的发生率高于TPN组(P < 0.05)。两组胆漏和手术部位感染的发生率无显著差异(P > 0.05)。
术后EEN方案可降低MOJ胆管癌患者术后并发症的发生率,改善临床结局和免疫功能,从而有利于患者康复。