Huang Chun-Ming, Huang Ching-Wen, Ma Cheng-Jen, Tsai Hsiang-Lin, Su Wei-Chih, Chang Tsung-Kun, Huang Ming-Yii, Wang Jaw Yuan
Department of Radiation Oncology, Kaohsiung Medical University Hospital, Kaohsiung 80145, Taiwan.
Department of Surgery, Kaohsiung Medical University Hospital, Kaohsiung Medical University, Kaohsiung 80145, Taiwan.
World J Gastrointest Oncol. 2020 Dec 15;12(12):1428-1442. doi: 10.4251/wjgo.v12.i12.1428.
Patients with clinical T4 colorectal cancer (CRC) have a poor prognosis because of compromised surgical margins. Neoadjuvant therapy may be effective in downstaging tumors, thereby rendering possible radical resection with clear margins.
To evaluate tumor downsizing and resection with clear margins in T4 CRC patients undergoing neoadjuvant concurrent chemoradiotherapy followed by surgery.
This study retrospectively included 86 eligible patients with clinical T4 CRC who underwent neoadjuvant concurrent chemoradiotherapy followed by radical resection. Neoadjuvant therapy consisted of radiation therapy at a dose of 45-50.4 Gy and chemotherapy agents, either FOLFOX or capecitabine. A circumferential resection margin (CRM) of < 1 mm was considered to be a positive margin. We defined pathological complete response (pCR) as the absence of any malignant cells in a specimen, including the primary tumor and lymph nodes. A multivariate logistic regression model was used to identify independent predictive factors for pCR.
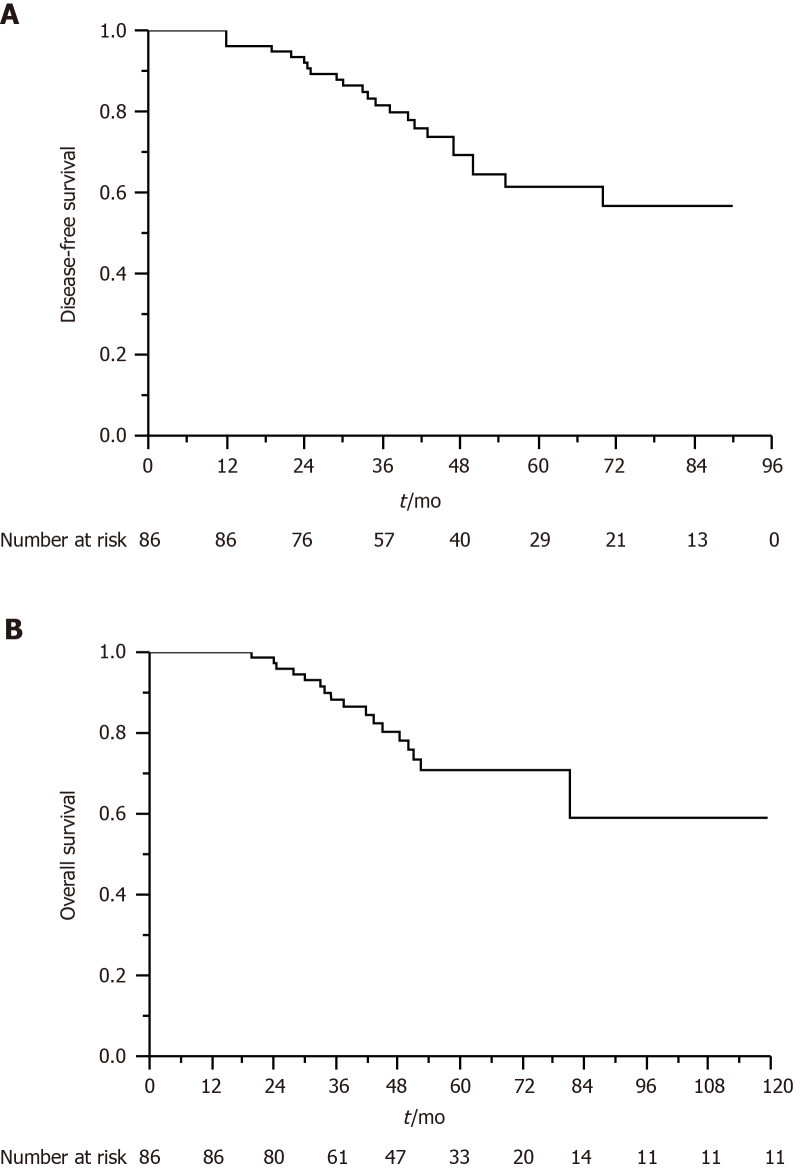
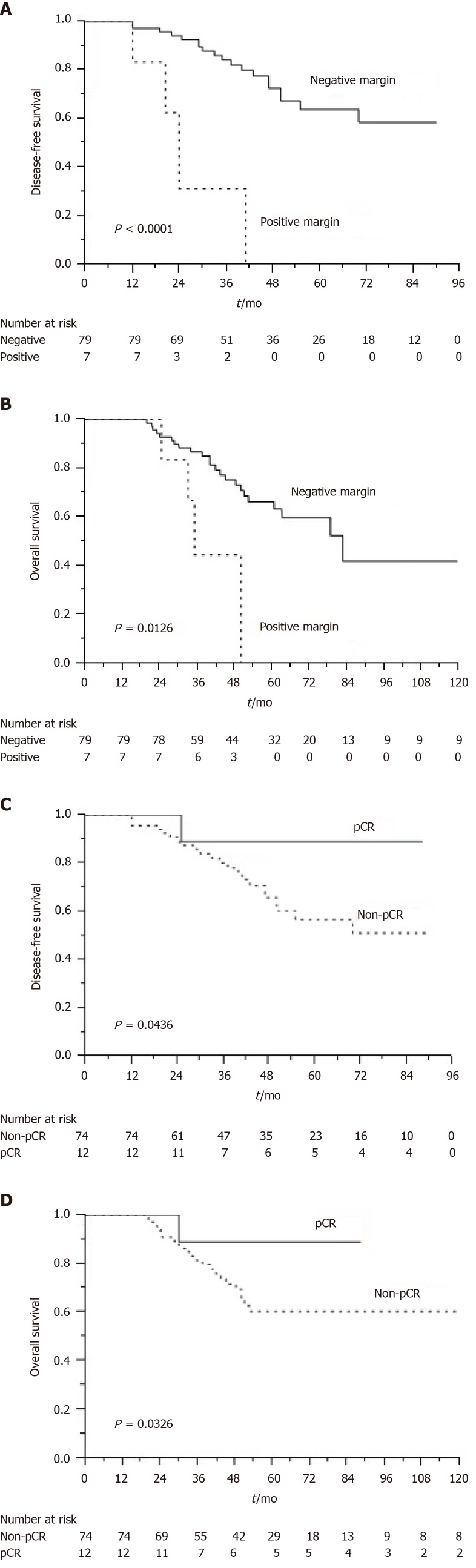
For 86 patients who underwent neoadjuvant chemoradiotherapy and surgery, the rate of pCR was 14%, and the R0 resection rate was 91.9%. Of the 61 patients with rectal cancer, 7 (11.5%) achieved pCR and 5 (8.2%) had positive CRMs. Of the 25 patients with colon cancer, 5 (20%) achieved pCR and 2 (8%) had positive CRMs. We observed that the FOLFOX regimen was an independent predictor of pCR ( = 0.046). After a median follow-up of 47 mo, the estimated 5-year overall survival (OS) and disease-free survival (DFS) rates were 70.8% and 61.4%, respectively. Multivariate analysis revealed that a tumor with a negative resection margin was associated with improved DFS ( = 0.014) and OS ( = 0.001). Patients who achieved pCR exhibited longer DFS ( = 0.042) and OS ( = 0.003) than those who did not.
Neoadjuvant concurrent chemoradiotherapy engenders favorable pCR and R0 resection rates among patients with T4 CRC. The R0 resection rate and pCR are independent prognostic factors for patients with T4 CRC.
临床T4期结直肠癌(CRC)患者由于手术切缘不理想,预后较差。新辅助治疗可能有效缩小肿瘤分期,从而实现切缘阴性的根治性切除。
评估接受新辅助同步放化疗后手术的T4期CRC患者的肿瘤缩小情况及切缘阴性切除率。
本研究回顾性纳入86例符合条件的临床T4期CRC患者,这些患者接受了新辅助同步放化疗后行根治性切除。新辅助治疗包括45 - 50.4 Gy的放射治疗和化疗药物,化疗方案为FOLFOX或卡培他滨。环周切缘(CRM)< 1 mm被认为是阳性切缘。我们将病理完全缓解(pCR)定义为标本中无任何恶性细胞,包括原发肿瘤和淋巴结。采用多因素逻辑回归模型确定pCR的独立预测因素。
86例接受新辅助放化疗和手术的患者中,pCR率为14%,R0切除率为91.9%。61例直肠癌患者中,7例(11.5%)达到pCR,5例(8.2%)CRM阳性。25例结肠癌患者中,5例(20%)达到pCR,2例(8%)CRM阳性。我们观察到FOLFOX方案是pCR的独立预测因素(P = 0.046)。中位随访47个月后,估计5年总生存率(OS)和无病生存率(DFS)分别为70.8%和61.4%。多因素分析显示,切缘阴性的肿瘤与DFS改善(P = 0.014)和OS改善(P = 0.001)相关。达到pCR的患者比未达到pCR的患者表现出更长的DFS(P = 0.042)和OS(P = 0.003)。
新辅助同步放化疗在T4期CRC患者中产生了良好的pCR率和R0切除率。R0切除率和pCR是T4期CRC患者的独立预后因素。