Peña-Oyarzún Daniel, Reyes Montserrat, Hernández-Cáceres María Paz, Kretschmar Catalina, Morselli Eugenia, Ramirez-Sarmiento Cesar A, Lavandero Sergio, Torres Vicente A, Criollo Alfredo
Advanced Center for Chronic Disease (ACCDiS), Facultad de Ciencias Químicas & Farmacéuticas and Facultad de Medicina, Universidad de Chile, Santiago, Chile.
Facultad de Odontología, Instituto de Investigación en Ciencias Odontológicas, Universidad de Chile, Santiago, Chile.
Front Oncol. 2020 Dec 9;10:602661. doi: 10.3389/fonc.2020.602661. eCollection 2020.
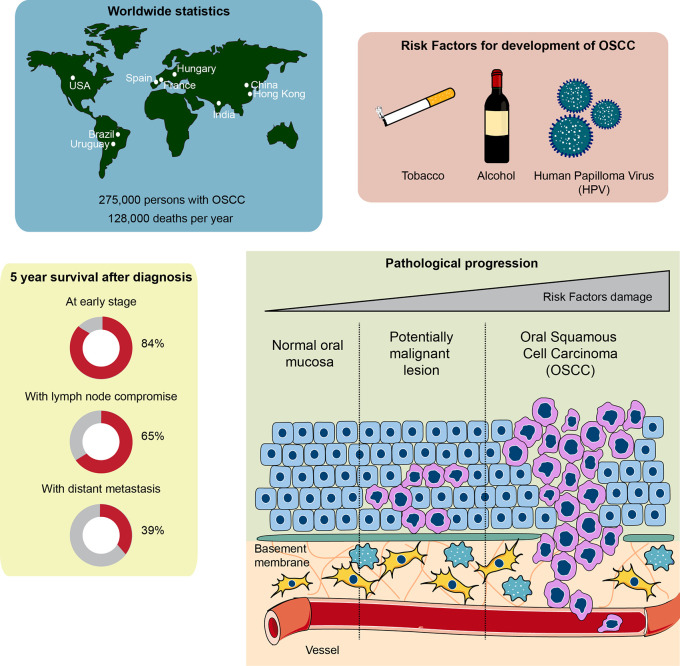
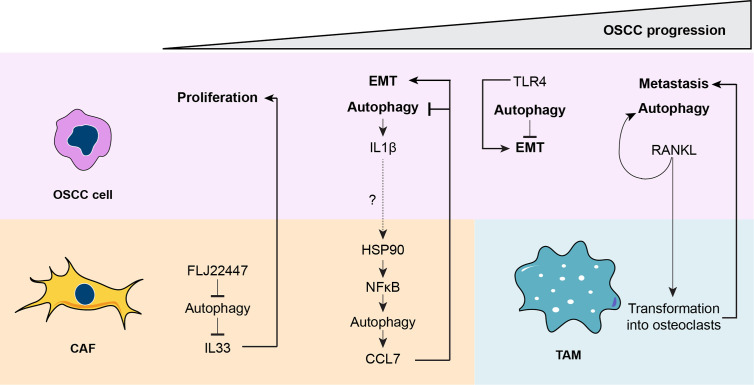
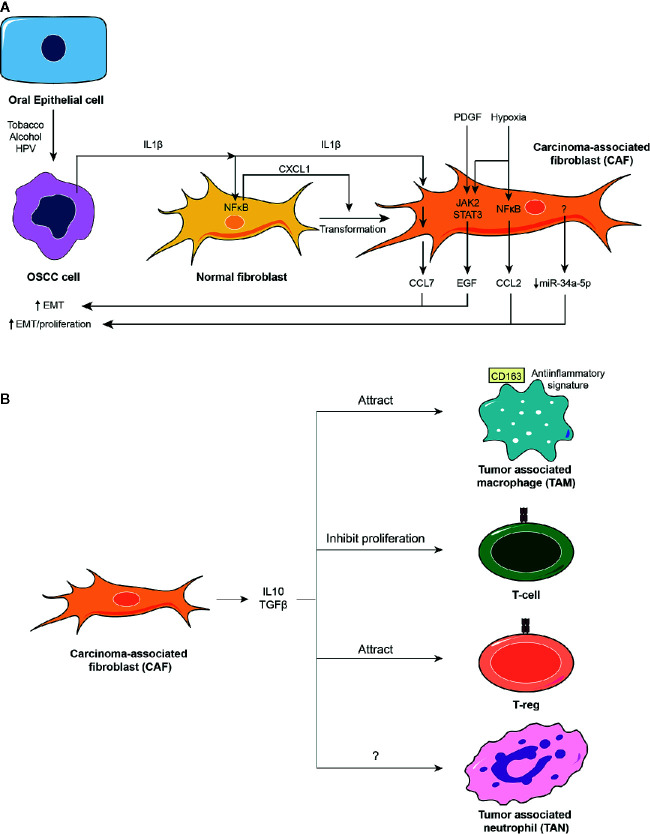
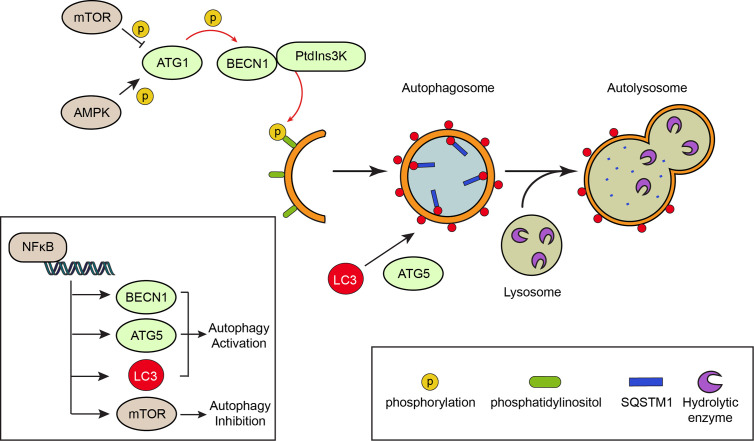
Oral squamous cell carcinoma, the most common type of oral cancer, affects more than 275,000 people per year worldwide. Oral squamous cell carcinoma is very aggressive, as most patients die after 3 to 5 years post-diagnosis. The initiation and progression of oral squamous cell carcinoma are multifactorial: smoking, alcohol consumption, and human papilloma virus infection are among the causes that promote its development. Although oral squamous cell carcinoma involves abnormal growth and migration of oral epithelial cells, other cell types such as fibroblasts and immune cells form the carcinoma niche. An underlying inflammatory state within the oral tissue promotes differential stress-related responses that favor oral squamous cell carcinoma. Autophagy is an intracellular degradation process that allows cancer cells to survive under stress conditions. Autophagy degrades cellular components by sequestering them in vesicles called autophagosomes, which ultimately fuse with lysosomes. Although several autophagy markers have been associated with oral squamous cell carcinoma, it remains unclear whether up- or down-regulation of autophagy favors its progression. Autophagy levels during oral squamous cell carcinoma are both timing- and cell-specific. Here we discuss how autophagy is required to establish a new cellular microenvironment in oral squamous cell carcinoma and how autophagy drives the phenotypic change of oral squamous cell carcinoma cells by promoting crosstalk between carcinoma cells, fibroblasts, and immune cells.
口腔鳞状细胞癌是口腔癌最常见的类型,全球每年有超过27.5万人受其影响。口腔鳞状细胞癌极具侵袭性,大多数患者在确诊后3至5年内死亡。口腔鳞状细胞癌的发生和发展是多因素的:吸烟、饮酒和人乳头瘤病毒感染是促使其发展的部分原因。尽管口腔鳞状细胞癌涉及口腔上皮细胞的异常生长和迁移,但其他细胞类型如成纤维细胞和免疫细胞也构成了癌龛。口腔组织内潜在的炎症状态会促进不同的应激相关反应,这些反应有利于口腔鳞状细胞癌。自噬是一种细胞内降解过程,使癌细胞能够在应激条件下存活。自噬通过将细胞成分隔离在称为自噬体的囊泡中来降解它们,这些囊泡最终与溶酶体融合。尽管几种自噬标记物已与口腔鳞状细胞癌相关联,但自噬的上调或下调是否有利于其进展仍不清楚。口腔鳞状细胞癌期间的自噬水平具有时间和细胞特异性。在此,我们讨论自噬如何在口腔鳞状细胞癌中建立新的细胞微环境,以及自噬如何通过促进癌细胞、成纤维细胞和免疫细胞之间的相互作用来驱动口腔鳞状细胞癌细胞的表型变化。