Odeyemi Yewande E, Herasevich Svetlana, Chalmers Sarah J, Barreto Erin F, Frank Ryan D, Gajic Ognjen O, Yadav Hemang
Division of Pulmonary and Critical Care Medicine, Mayo Clinic, Rochester, MN.
Department of Pharmacy, Mayo Clinic, Rochester, MN.
Mayo Clin Proc Innov Qual Outcomes. 2020 Dec 10;4(6):649-656. doi: 10.1016/j.mayocpiqo.2020.07.011. eCollection 2020 Dec.
To evaluate the frequency and consequences of prescribing corticosteroids for pneumonia in a biomarker-concordant manner.
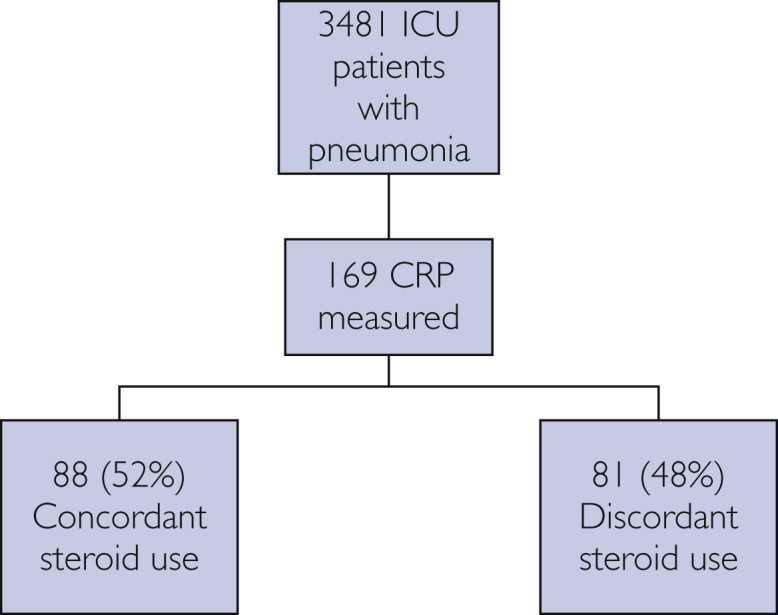
This was a single-center retrospective cohort study of adults with pneumonia admitted to the medical intensive care unit (ICU) at Mayo Clinic in Rochester, Minnesota, between January 1, 2009, and June 30, 2014. Steroid use was "biomarker concordant" if given when C-reactive protein (CRP) was ≥150 mg/L or withheld when CRP was <150 mg/L, and vice versa for biomarker discordant.
Of 3481 ICU admissions with community-acquired pneumonia, 169 (4.9%) had CRPs measured within 48 hours of admission to the ICU. Steroid use in the ICU was biomarker concordant in 88 (52%) patients and biomarker discordant in 81 (48%) patients. Biomarker-concordant steroid use was associated with faster resolution of lung injury: median fraction of inspired oxygen on day 3 (0.4 [0.3, 0.5] vs 0.3 [0.21, 0.4], =.005), day 4 (0.35 [0.3, 0.5] vs 0.28 [0.21, 0.38], =<.001), and day 5 (0.30 [0.24, 0.45] vs 0.28 [0.21, 0.40], =.03), and increased ICU (3.5; 95% CI, 0.5 to 6.4, =.02), and hospital-free days (3.6; 95% CI, 0.4 to 6.8, =.03) on multivariate analysis.
In critically ill patients with community-acquired pneumonia, steroid use is rarely biomarker informed and often discordant with inflammatory biomarker levels. Biomarker-concordant steroid use was associated with a faster recovery of hypoxemia and increased ICU- and hospital-free days. Future well-designed prospective studies are justified to test the potential value of biomarker-concordant steroid therapy.
以生物标志物相符的方式评估肺炎患者使用皮质类固醇的频率及后果。
这是一项对2009年1月1日至2014年6月30日期间入住明尼苏达州罗切斯特市梅奥诊所医学重症监护病房(ICU)的成年肺炎患者进行的单中心回顾性队列研究。如果在C反应蛋白(CRP)≥150 mg/L时给予类固醇,则类固醇使用为“生物标志物相符”,而当CRP<150 mg/L时停用类固醇,反之则为生物标志物不相符。
在3481例因社区获得性肺炎入住ICU的患者中,169例(4.9%)在入住ICU后48小时内检测了CRP。88例(52%)患者在ICU使用类固醇时生物标志物相符,81例(48%)患者生物标志物不相符。生物标志物相符的类固醇使用与肺损伤更快缓解相关:第3天吸入氧分数中位数(0.4 [0.3, 0.5] 对 0.3 [0.21, 0.4],P = 0.005)、第4天(0.35 [0.3, 0.5] 对 0.28 [0.21, 0.38],P < 0.001)和第5天(0.30 [0.24, 0.45] 对 0.28 [0.21, 0.40],P = 0.03),多因素分析显示ICU无日数增加(3.5;95%可信区间,0.5至6.4,P = 0.02),住院无日数增加(3.6;95%可信区间,0.4至6.8,P = 0.03)。
在患有社区获得性肺炎的重症患者中,类固醇的使用很少依据生物标志物,且常常与炎症生物标志物水平不相符。生物标志物相符的类固醇使用与低氧血症更快恢复以及ICU无日数和住院无日数增加相关。未来有必要开展精心设计的前瞻性研究来检验生物标志物相符的类固醇治疗的潜在价值。