Lu Zhiwei, Cheng Yusheng, Tu Xiongwen, Chen Liang, Chen Hu, Yang Jian, Wang Jinyan, Zhang Liqin
Department of Respiratory Medicine, Yijishan Hospital of Wannan Medical College, Wuhu, People's Republic of China.
Int J Chron Obstruct Pulmon Dis. 2016 Aug 9;11:1867-72. doi: 10.2147/COPD.S113510. eCollection 2016.
The aim of this study was to appraise the effect of community-acquired pneumonia (CAP) on inhospital mortality in critically ill acute exacerbation of COPD (AECOPD) patients admitted to a respiratory intensive care unit.
A retrospective observational study was performed. Consecutive critically ill AECOPD patients receiving treatment in a respiratory intensive care unit were reviewed from September 1, 2012, to August 31, 2015. Categorical variables were analyzed using chi-square tests, and continuous variables were analyzed by Mann-Whitney U-test. Kaplan-Meier analysis was used to assess the association of CAP with survival of critically ill AECOPD patients for univariate analysis. Cox's proportional hazards regression model was performed to identify risk factors for multivariate analysis.
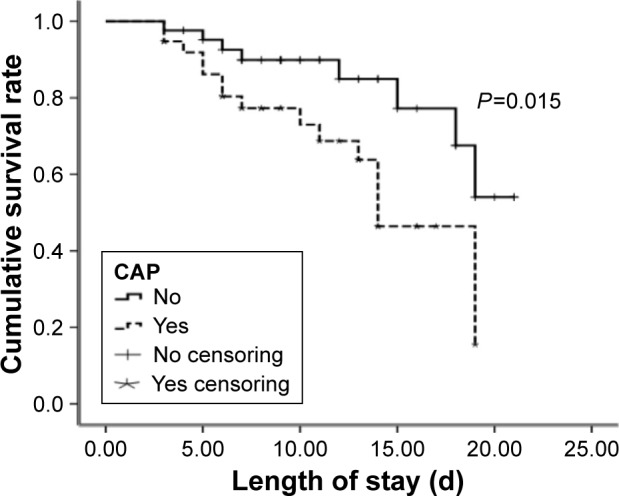
A total of 80 consecutive eligible individuals were reviewed. These included 38 patients with CAP and 42 patients without CAP. Patients with CAP had a higher inhospital rate of mortality than patients without CAP (42% vs 33.3%, P<0.05). Kaplan-Meier survival analysis showed that patients with CAP had a worse survival rate than patients without CAP (P<0.05). Clinical characteristics, including Acute Physiology and Chronic Health Evaluation II (APACHE II) score, C-reactive protein, and CAP, were found to be closely associated with survival of AECOPD individuals. Further multivariate Cox regression analysis confirmed that CAP and APACHE II were independent risk factors for inhospital mortality in critically ill AECOPD patients (CAP: hazard ratio, 5.29; 95% CI, 1.50-18.47, P<0.01 and APACHE II: hazard ratio, 1.20; 95% CI, 1.06-1.37, P<0.01).
CAP may be an independent risk factor for higher inhospital mortality in critically ill AECOPD patients.
本研究旨在评估社区获得性肺炎(CAP)对入住呼吸重症监护病房的慢性阻塞性肺疾病急性加重期(AECOPD)危重症患者院内死亡率的影响。
进行了一项回顾性观察研究。对2012年9月1日至2015年8月31日期间在呼吸重症监护病房接受治疗的连续性AECOPD危重症患者进行了回顾。分类变量采用卡方检验进行分析,连续变量采用曼-惠特尼U检验进行分析。采用Kaplan-Meier分析评估CAP与AECOPD危重症患者生存情况的相关性,进行单因素分析。采用Cox比例风险回归模型确定多因素分析的危险因素。
共回顾了80例连续符合条件的个体。其中包括38例CAP患者和42例无CAP患者。CAP患者的院内死亡率高于无CAP患者(42%对33.3%,P<0.05)。Kaplan-Meier生存分析显示,CAP患者的生存率低于无CAP患者(P<0.05)。发现包括急性生理与慢性健康状况评分系统II(APACHE II)评分、C反应蛋白和CAP在内的临床特征与AECOPD患者的生存密切相关。进一步的多因素Cox回归分析证实,CAP和APACHE II是AECOPD危重症患者院内死亡 的独立危险因素(CAP:风险比,5.29;95%置信区间,1.50 - 18.47,P<0.01;APACHE II:风险比,1.20;95%置信区间,1.06 - 1.37,P<0.01)。
CAP可能是AECOPD危重症患者院内死亡率升高的独立危险因素。