Pediatric Endocrinology, Diabetology, and Metabolism, Inselspital, Bern University Hospital, University of Bern, Bern, Switzerland.
Department of Pediatric Surgery, Inselspital, Bern University Hospital, University of Bern, Bern, Switzerland.
J Clin Endocrinol Metab. 2021 Apr 23;106(5):1530-1539. doi: 10.1210/clinem/dgaa948.
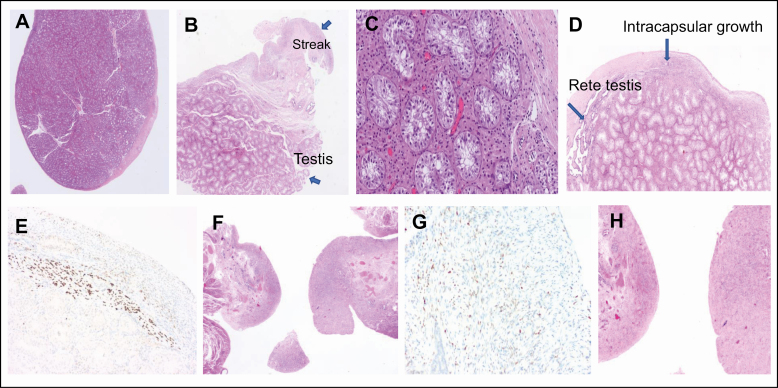
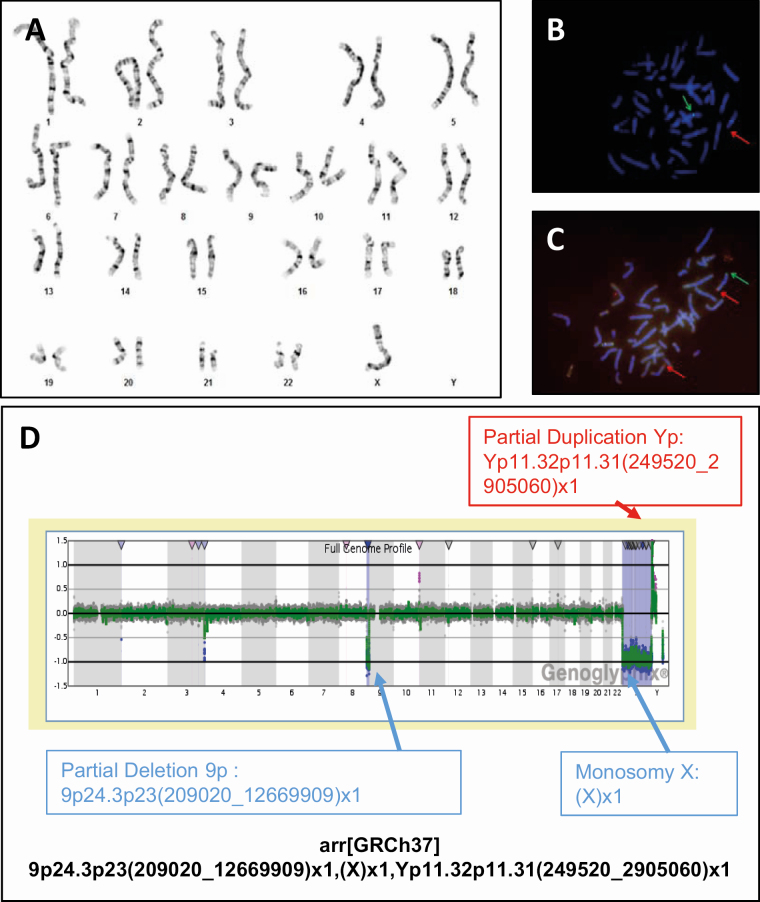
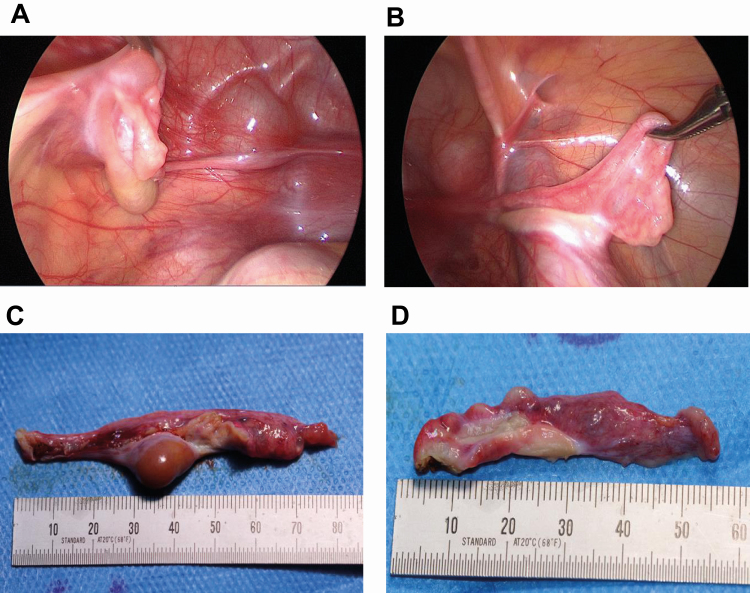
Virilization is the medical term for describing a female who develops characteristics associated with male hormones (androgens) at any age, or when a newborn girl shows signs of prenatal male hormone exposure at birth. In girls, androgen levels are low during pregnancy and childhood. A first physiologic rise of adrenal androgens is observed at the age of 6 to 8 years and reflects functional activation of the zona reticularis of the adrenal cortex at adrenarche, manifesting clinically with first pubic and axillary hairs. Early adrenarche is known as "premature adrenarche." It is mostly idiopathic and of uncertain pathologic relevance but requires the exclusion of other causes of androgen excess (eg, nonclassic congenital adrenal hyperplasia) that might exacerbate clinically into virilization. The second modest physiologic increase of circulating androgens occurs then during pubertal development, which reflects the activation of ovarian steroidogenesis contributing to the peripheral androgen pool. However, at puberty initiation (and beyond), ovarian steroidogenesis is normally devoted to estrogen production for the development of secondary female bodily characteristics (eg, breast development). Serum total testosterone in a young adult woman is therefore about 10- to 20-fold lower than in a young man, whereas midcycle estradiol is about 10- to 20-fold higher. But if androgen production starts too early, progresses rapidly, and in marked excess (usually more than 3 to 5 times above normal), females will manifest with signs of virilization such as masculine habitus, deepening of the voice, severe acne, excessive facial and (male typical) body hair, clitoromegaly, and increased muscle development. Several medical conditions may cause virilization in girls and women, including androgen-producing tumors of the ovaries or adrenal cortex, (non)classical congenital adrenal hyperplasia and, more rarely, other disorders (also referred to as differences) of sex development (DSD). The purpose of this article is to describe the clinical approach to the girl with virilization at puberty, focusing on diagnostic challenges. The review is written from the perspective of the case of an 11.5-year-old girl who was referred to our clinic for progressive, rapid onset clitoromegaly, and was then diagnosed with a complex genetic form of DSD that led to abnormal testosterone production from a dysgenetic gonad at onset of puberty. Her genetic workup revealed a unique translocation of an abnormal duplicated Y-chromosome to a deleted chromosome 9, including the Doublesex and Mab-3 Related Transcription factor 1 (DMRT1) gene.
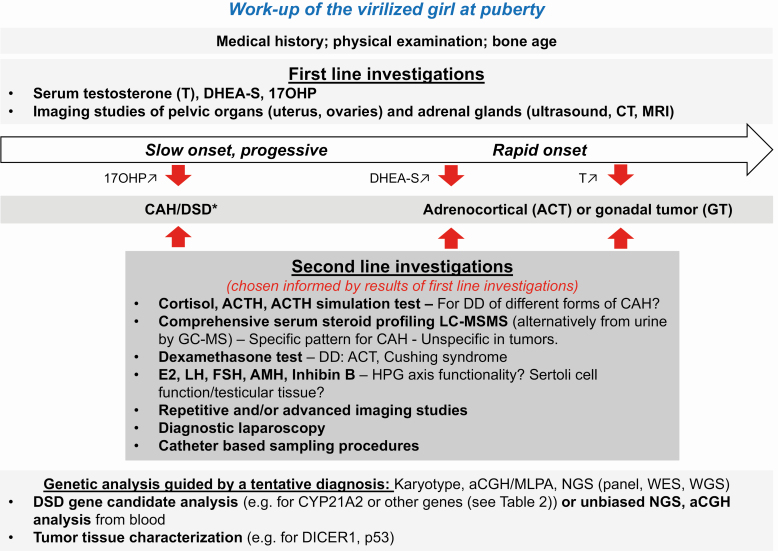
Identify the precise pathophysiologic mechanisms leading to virilization in girls at puberty considering that virilization at puberty may be the first manifestation of an endocrine active tumor or a disorder/difference of sex development (DSD) that remained undiagnosed before and may be life-threatening. Of the DSDs, nonclassical congenital adrenal hyperplasia occurs most often.Provide a step-by-step diagnostic workup plan including repeated and expanded biochemical and genetic tests to solve complex cases.Manage clinical care of a girl virilizing at puberty using an interdisciplinary team approach.Care for complex cases of DSD manifesting at puberty, such as the presented girl with a Turner syndrome-like phenotype and virilization resulting from a complex genetic variation.
描述青春期出现性早熟的女孩的临床处理方法,重点介绍诊断方面的挑战。本文基于一位 11.5 岁女孩的病例展开,她因阴蒂逐渐增大而就诊于我院,被诊断为一种复杂的遗传性性别发育差异(DSD),导致青春期时从发育不良的性腺开始异常产生睾酮。其基因检测发现一个独特的异常 Y 染色体与缺失的 9 号染色体易位,其中包括双性和 mab-3 相关转录因子 1(DMRT1)基因。
考虑到青春期性早熟可能是内分泌活跃肿瘤或性别发育障碍/差异(DSD)的首发表现,这些疾病在发病前可能未被诊断,且可能危及生命,因此要明确导致青春期女孩性早熟的确切病理生理机制。在 DSD 中,最常见的是非经典型先天性肾上腺增生。提供包括重复和扩展的生化和遗传检测在内的逐步诊断方案,以解决复杂病例。采用多学科团队方法管理青春期出现性早熟的女孩的临床护理。处理青春期表现出的复杂 DSD 病例,如本例特纳综合征样表型和由复杂遗传变异引起的性早熟。