Department of Laboratory Medicine and Pathology, Mayo Clinic, Rochester, Minnesota, USA.
Department of Neurology, Mayo Clinic, Rochester, Minnesota, USA.
Ann Clin Transl Neurol. 2021 Feb;8(2):425-439. doi: 10.1002/acn3.51284. Epub 2020 Dec 28.
To describe CSF-defined neuronal intermediate filament (NIF) autoimmunity.
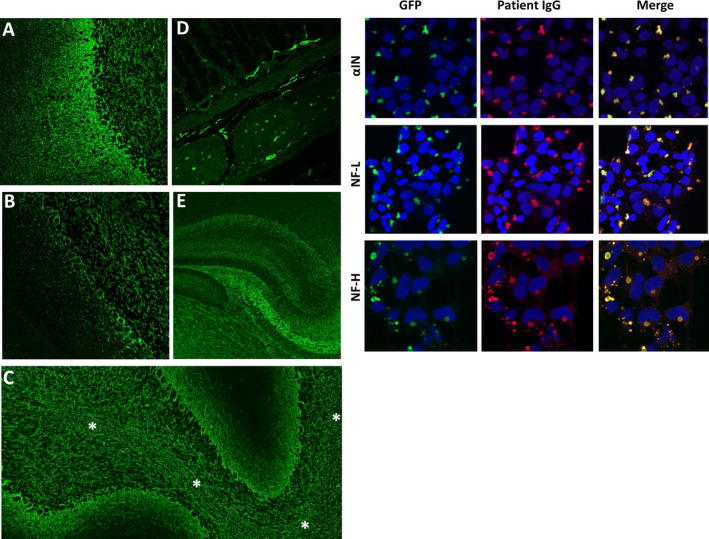
NIF-IgG CSF-positive patients (41, 0.03% of 118599 tested, 1996-2019) were included (serum was neither sensitive nor specific). Criteria-based patient NIF-IgG staining of brain and myenteric NIFs was detected by indirect immunofluorescence assay (IFA); NIF-specificity was confirmed by cell-based assays (CBAs, alpha internexin, neurofilament light [NF-L]), heavy-[NF-H] chain).
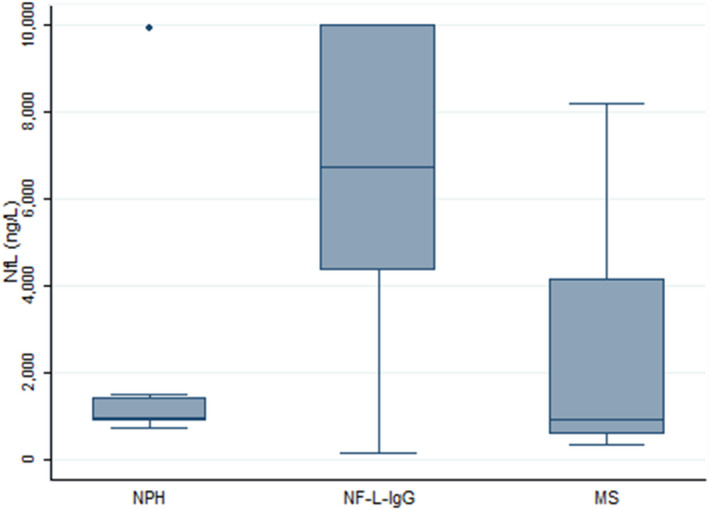
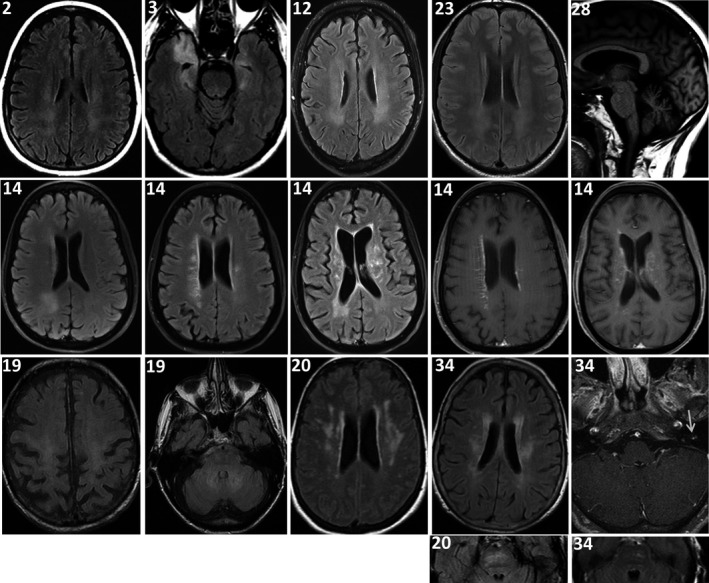
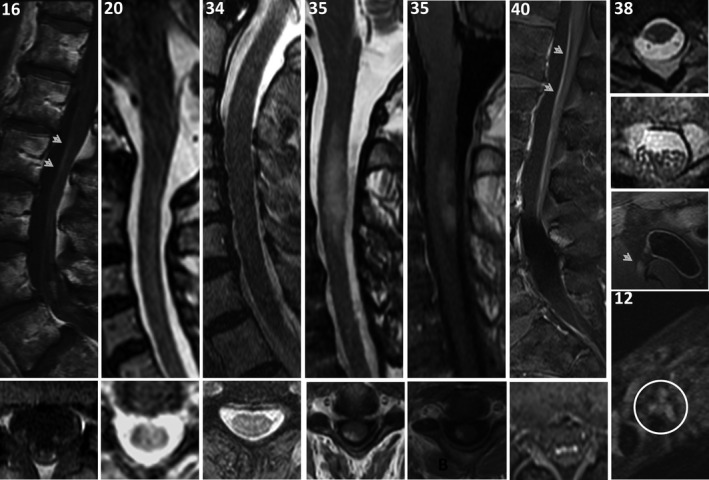
Sixty-one percent of 41 patients were men, median age, 61 years (range, 21-88). Syndromes were encephalopathy predominant (23), cerebellar ataxia predominant (11), or myeloradiculoneuropathies (7). MRI abnormalities (T2 hyperintensities of brain, spinal cord white matter tracts. and peripheral nerve axons) and neurophysiologic testing (EEG, EMG, evoked potentials) co-localized with clinical neurological phenotypes (multifocal in 29%). Thirty patients (73%) had ≥ 1 immunological perturbation: cancer (paraneoplastic), 22; systemic infection (parainfectious [including ehrlichosis, 3] or HIV), 7; checkpoint-inhibitor cancer immunotherapy, 4; other, 5. Cancers were as follows: neuroendocrine-lineage carcinomas, 12 (small cell, 6; Merkel cell, 5; pancreatic, 1 [11/12 had NF-L-IgG detected, versus 8/29 others, P = 0.0005]) and other, 11. Onset was predominantly subacute (92%) and accompanied by inflammatory CSF (75%), and immunotherapy response (77%). In contrast, CSF controls (15684 total) demonstrated NIF-IgG negativity (100% of test validation controls), and low frequencies of autoimmune diagnoses (20% of consecutively referred clinical specimens) and neuroendocrine-lineage carcinoma diagnosis (3.1% vs. 30% of NIF cases), P < 0.0001. Median NF-L protein concentration was higher in 8 NF-L-IgG-positive patients (median, 6718 ng/L) than 16 controls.
Neurological autoimmunity, defined by CSF-detected NIF-IgGs, represents a continuum of treatable axonopathies, sometimes paraneoplastic or parainfectious.
描述脑脊液中神经元中间丝(NIF)自身抗体。
纳入 NIF-IgG 脑脊液阳性患者(41 例,占 1996-2019 年检测的 118599 例患者的 0.03%)(血清既不敏感也不特异)。通过间接免疫荧光法(IFA)检测脑和肌间 NIF 患者的基于标准的 NIF-IgG 染色;通过基于细胞的检测(CBA、α中间丝蛋白、神经丝轻链 [NF-L]、重链 [NF-H])确认 NIF 的特异性。
41 例患者中 61%为男性,中位年龄为 61 岁(范围为 21-88 岁)。综合征以脑病为主(23 例)、小脑共济失调为主(11 例)或脊神经根神经病(7 例)。MRI 异常(脑、脊髓白质束和周围神经轴突的 T2 高信号)和神经生理学检查(EEG、EMG、诱发电位)与临床神经表型一致(29%为多灶性)。30 例(73%)患者存在≥1 种免疫异常:癌症(副肿瘤性)22 例;全身感染(副感染性[包括埃立克体病,3 例]或 HIV)7 例;检查点抑制剂癌症免疫治疗 4 例;其他 5 例。癌症如下:神经内分泌谱系癌 12 例(小细胞癌 6 例;默克尔细胞癌 5 例;胰腺 1 例[11/12 例检测到 NF-L-IgG,而其他 29 例中 8 例,P=0.0005])和其他 11 例。发病主要为亚急性(92%),伴有炎症性 CSF(75%)和免疫治疗反应(77%)。相比之下,脑脊液对照(15684 个总标本)表现为 NIF-IgG 阴性(100%的检测验证对照),自身免疫性疾病诊断频率较低(连续转诊的临床标本的 20%)和神经内分泌谱系癌诊断频率较低(3.1%比 NIF 病例的 30%),P<0.0001。在 8 例 NF-L-IgG 阳性患者(中位数,6718ng/L)中,NF-L 蛋白浓度中位数高于 16 例对照。
由 CSF 检测到的 NIF-IgG 定义的神经自身免疫反应,代表了一种可治疗的轴突病谱,有时为副肿瘤性或副感染性。