Research School of Population Health, Australian National University, Canberra, Australia.
Neglected Tropical Diseases Support Center, Task Force for Global Heath, Decatur, Georgia, United States of America.
PLoS Negl Trop Dis. 2020 Dec 28;14(12):e0008916. doi: 10.1371/journal.pntd.0008916. eCollection 2020 Dec.
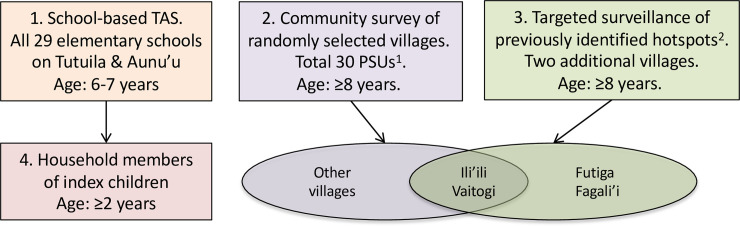
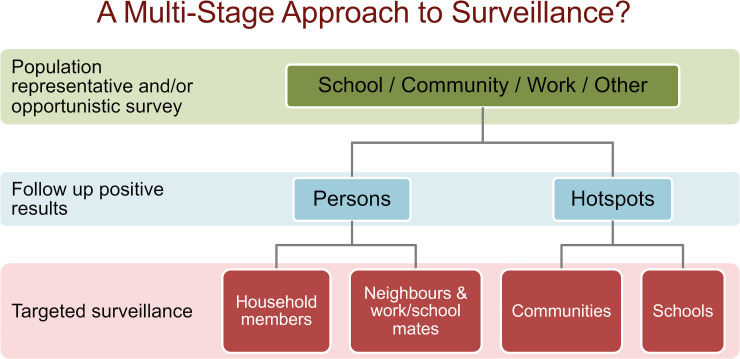
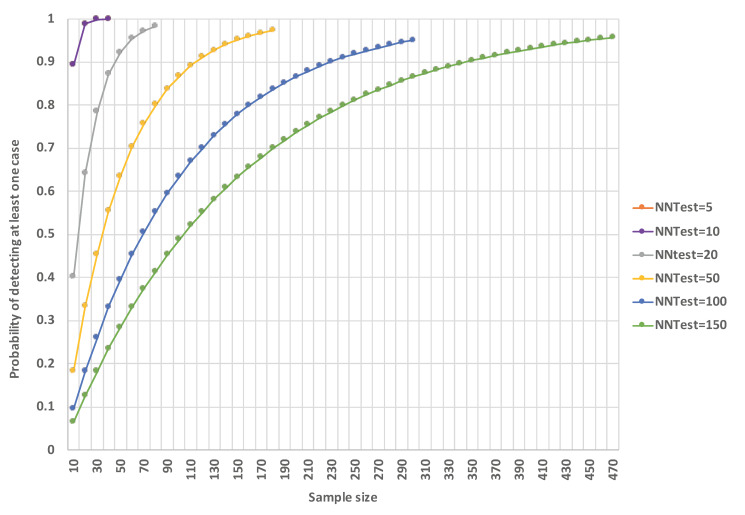
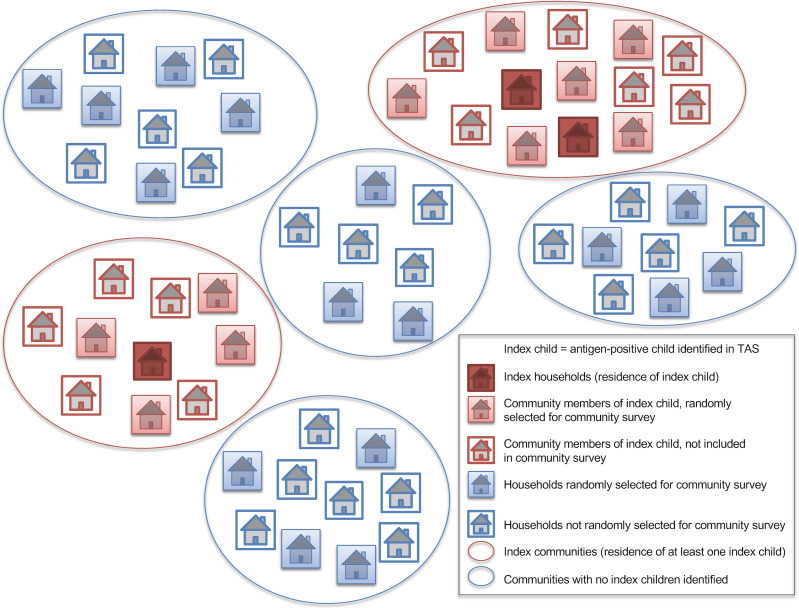
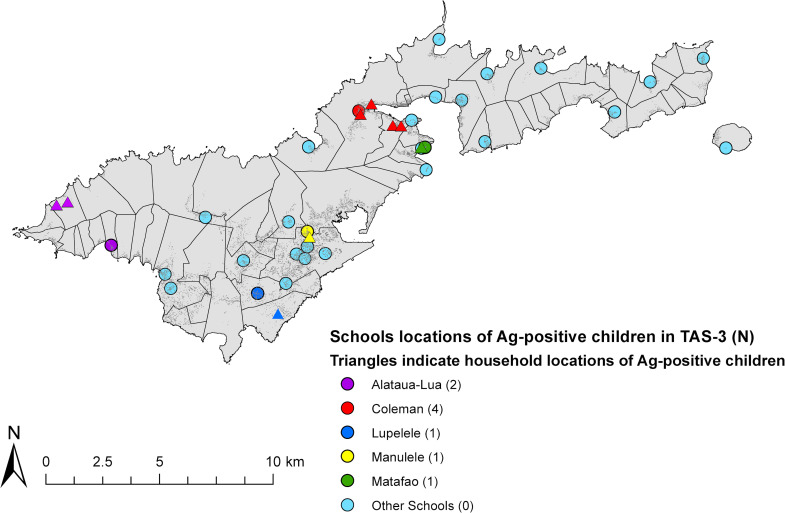
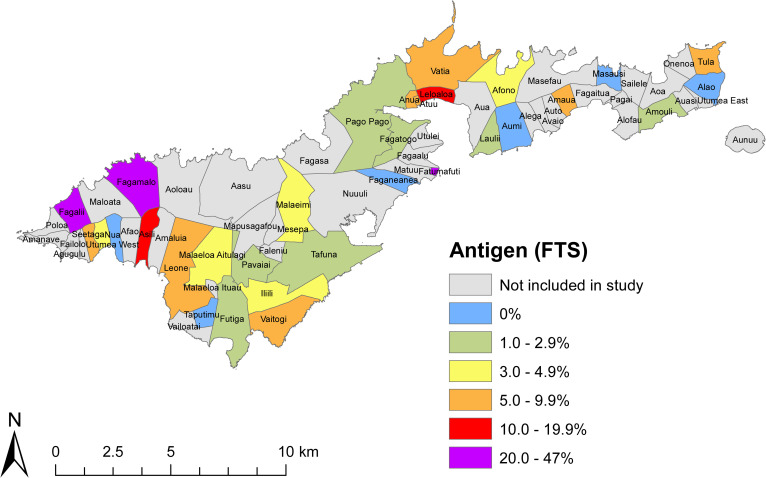
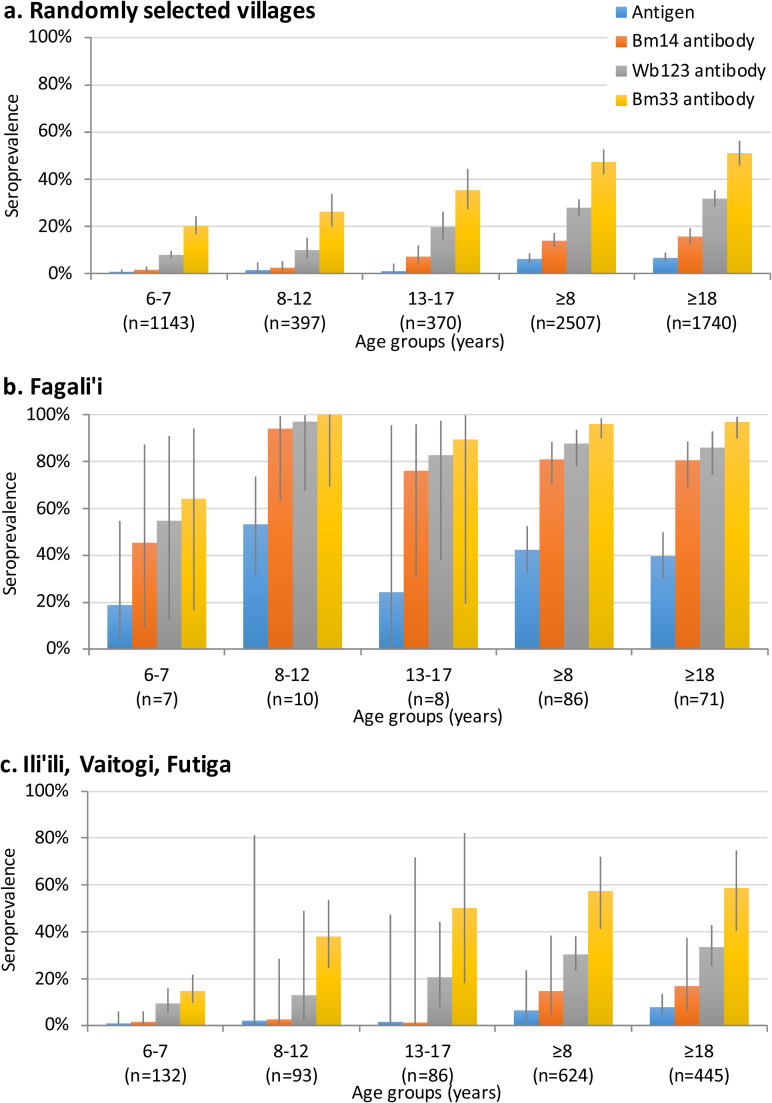
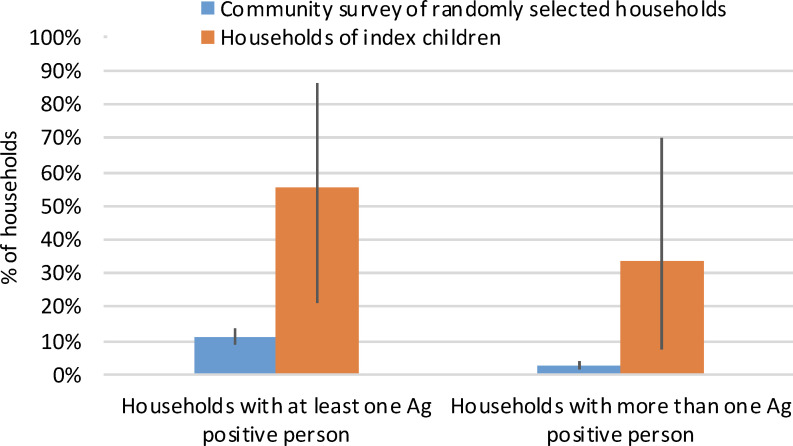
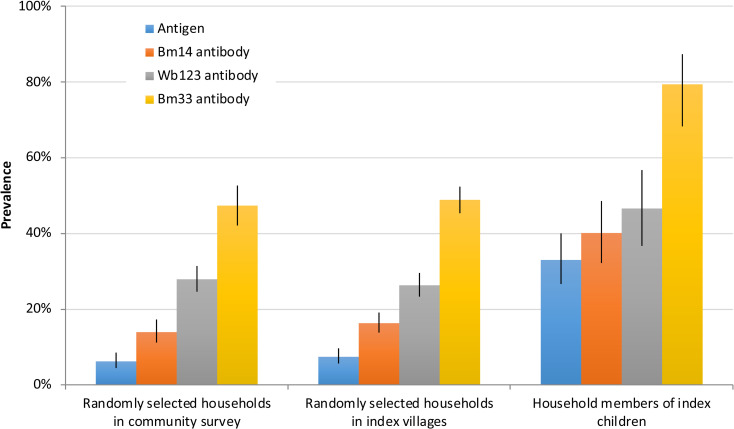
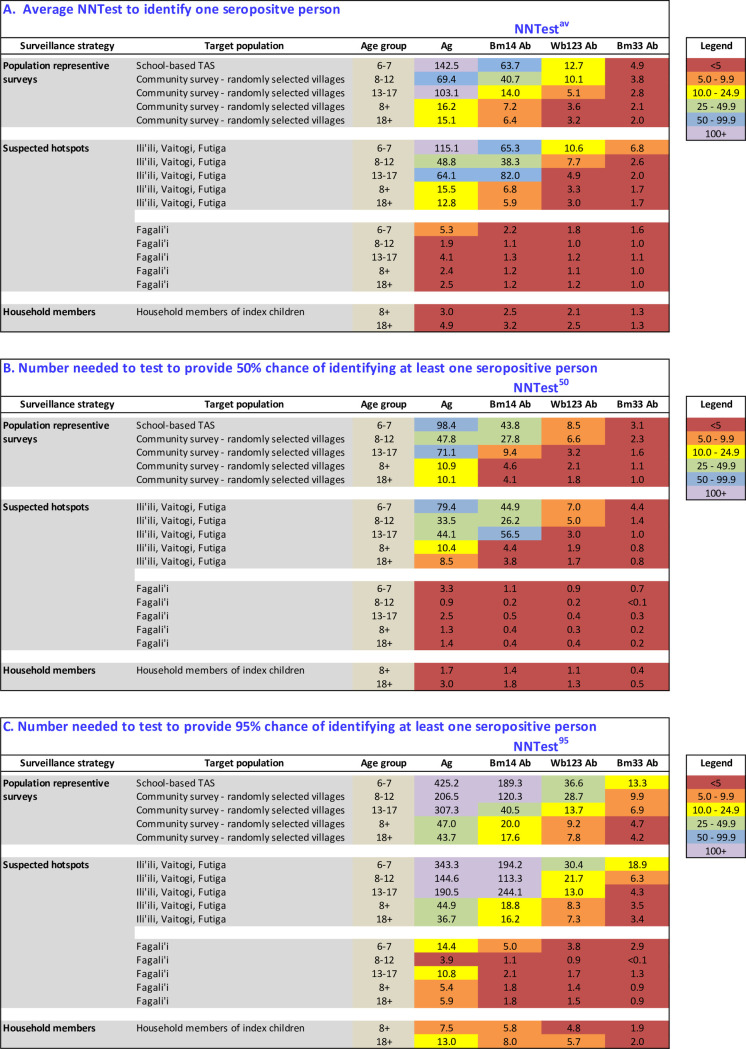
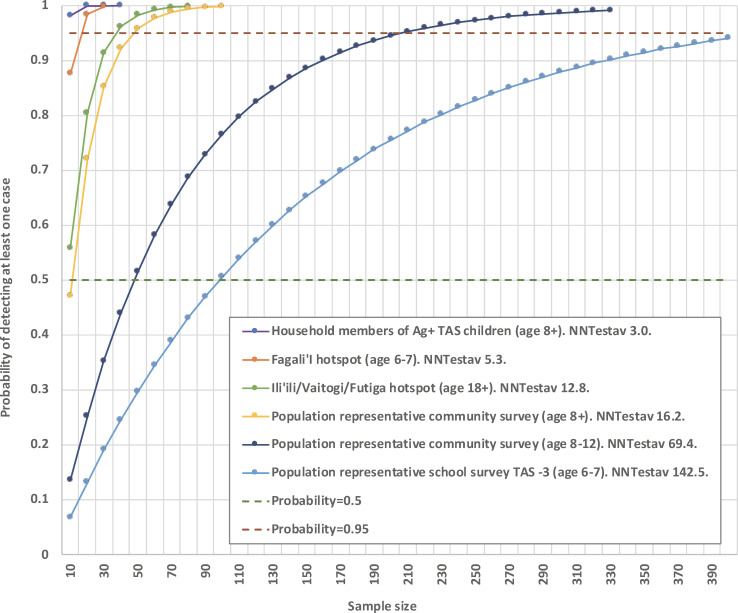
Under the Global Programme to Eliminate Lymphatic Filariasis (LF), American Samoa conducted mass drug administration (MDA) from 2000-2006. Despite passing Transmission Assessment Surveys (TAS) in 2011/2012 and 2015, American Samoa failed TAS-3 in 2016, with antigen (Ag) prevalence of 0.7% (95%CI 0.3-1.8%) in 6-7 year-olds. A 2016 community survey (Ag prevalence 6.2% (95%CI 4.4-8.5%) in age ≥8 years) confirmed resurgence. Using data from the 2016 survey, this study aims to i) investigate antibody prevalence in TAS-3 and the community survey, ii) identify risk factors associated with being seropositive for Ag and anti-filarial antibodies, and iii) compare the efficiency of different sampling strategies for identifying seropositive persons in the post-MDA setting. Antibody prevalence in TAS-3 (n = 1143) were 1.6% for Bm14 (95%CI 0.9-2.9%), 7.9% for Wb123 (95%CI 6.4-9.6%), and 20.2% for Bm33 (95%CI 16.7-24.3%); and in the community survey (n = 2507), 13.9% for Bm14 (95%CI 11.2-17.2%), 27.9% for Wb123 (95%CI 24.6-31.4%), and 47.3% for Bm33 (95%CI 42.1-52.6%). Multivariable logistic regression was used to identify risk factors for being seropositive for Ag and antibodies. Higher Ag prevalence was found in males (adjusted odds ratio [aOR] 3.01), age ≥18 years (aOR 2.18), residents of Fagali'i (aOR 15.81), and outdoor workers (aOR 2.61). Ag prevalence was 20.7% (95%CI 9.7-53.5%) in households of Ag-positive children identified in TAS-3. We used NNTestav (average number needed to test to identify one positive) to compare the efficiency of the following strategies for identifying persons who were seropositive for Ag and each antibody: i) TAS of 6-7 year-old children, ii) population representative surveys of older age groups, and iii) targeted surveillance of subpopulations at higher risk of being seropositive (older ages, householders of Ag-positive TAS children, and known hotspots). For Ag, NNTestav ranged from 142.5 for TAS, to <5 for households of index children. NNTestav was lower in older ages, and highest for Ag, followed by Bm14, Wb123 and Bm33 antibodies. We propose a multi-stage surveillance strategy, starting with population-representative sampling (e.g. TAS or population representative survey of older ages), followed by strategies that target subpopulations and/or locations with low NNTestav. This approach could potentially improve the efficiency of identifying remaining infected persons and residual hotspots. Surveillance programs should also explore the utility of antibodies as indicators of transmission.
在全球消灭淋巴丝虫病计划(LF)下,美属萨摩亚于 2000-2006 年进行了大规模药物治疗(MDA)。尽管在 2011/2012 年和 2015 年通过了传播评估调查(TAS),但美属萨摩亚在 2016 年的 TAS-3 中失败了,6-7 岁儿童的抗原(Ag)患病率为 0.7%(95%CI 0.3-1.8%)。2016 年的社区调查(≥8 岁人群的 Ag 患病率为 6.2%(95%CI 4.4-8.5%))证实了疫情的再次出现。利用 2016 年调查的数据,本研究旨在:i)调查 TAS-3 和社区调查中的抗体流行率,ii)确定与 Ag 和抗丝虫抗体呈阳性相关的风险因素,以及 iii)比较不同抽样策略在 MDA 后环境中识别血清阳性者的效率。TAS-3 中的抗体流行率(n=1143)为:Bm14 为 1.6%(95%CI 0.9-2.9%),Wb123 为 7.9%(95%CI 6.4-9.6%),Bm33 为 20.2%(95%CI 16.7-24.3%);在社区调查(n=2507)中,Bm14 为 13.9%(95%CI 11.2-17.2%),Wb123 为 27.9%(95%CI 24.6-31.4%),Bm33 为 47.3%(95%CI 42.1-52.6%)。多变量逻辑回归用于确定 Ag 和抗体呈阳性的风险因素。Ag 患病率较高的人群为男性(调整后的优势比[aOR]3.01)、年龄≥18 岁(aOR 2.18)、法加里伊(Fagali'i)居民(aOR 15.81)和户外工作者(aOR 2.61)。在 TAS-3 中发现的 Ag 阳性儿童的家庭中,Ag 患病率为 20.7%(95%CI 9.7-53.5%)。我们使用 NNTestav(识别一个阳性者所需的平均检测次数)比较了以下策略识别 Ag 和每种抗体呈阳性者的效率:i)6-7 岁儿童的 TAS,ii)年龄较大人群的代表性人群调查,以及 iii)高危亚人群的靶向监测(年龄较大、Ag 阳性 TAS 儿童的家庭户主和已知热点地区)。对于 Ag,NNTestav 范围从 TAS 的 142.5 到索引儿童家庭的<5。NNTestav 在年龄较大时较低,Ag 最高,其次是 Bm14、Wb123 和 Bm33 抗体。我们提出了一种多阶段监测策略,从代表性人群抽样(例如 TAS 或年龄较大人群的代表性人群调查)开始,然后是针对亚人群和/或低 NNTestav 地点的策略。这种方法有可能提高识别剩余感染者和残留热点的效率。监测计划还应探索抗体作为传播指标的效用。