Department of Clinical Epidemiology, Leiden University Medical Center, Leiden, The Netherlands.
Department of Clinical Science, Intervention and Technology, Karolinska Institute, Stockholm, Sweden.
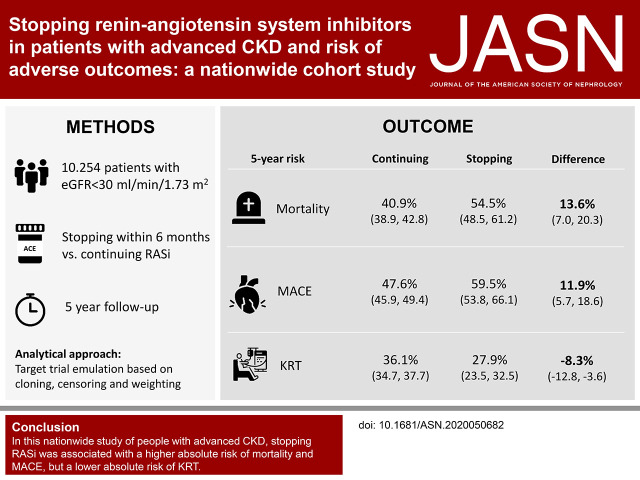
J Am Soc Nephrol. 2021 Feb;32(2):424-435. doi: 10.1681/ASN.2020050682. Epub 2020 Dec 28.
It is unknown whether stopping renin-angiotensin system (RAS) inhibitor therapy in patients with advanced CKD affects outcomes.
We studied patients referred to nephrologist care, listed on the Swedish Renal Registry during 2007-2017, who developed advanced CKD (eGFR<30 ml/min per 1.73 m) while on RAS inhibitor therapy. Using target trial emulation techniques on the basis of cloning, censoring, and weighting, we compared the risks of stopping within 6 months and remaining off treatment versus continuing RAS inhibitor therapy. These included risks of subsequent 5-year all-cause mortality, major adverse cardiovascular events, and initiation of kidney replacement therapy (KRT).
Of 10,254 prevalent RAS inhibitor users (median age 72 years, 36% female) with new-onset eGFR <30 ml/min per 1.73 m, 1553 (15%) stopped RAS inhibitor therapy within 6 months. Median eGFR was 23 ml/min per 1.73 m. Compared with continuing RAS inhibition, stopping this therapy was associated with a higher absolute 5-year risk of death (40.9% versus 54.5%) and major adverse cardiovascular events (47.6% versus 59.5%), but with a lower risk of KRT (36.1% versus 27.9%); these corresponded to absolute risk differences of 13.6 events per 100 patients, 11.9 events per 100 patients, and -8.3 events per 100 patients, respectively. Results were consistent whether patients stopped RAS inhibition at higher or lower eGFR, across prespecified subgroups, after adjustment and stratification for albuminuria and potassium, and when modeling RAS inhibition as a time-dependent exposure using a marginal structural model.
In this nationwide observational study of people with advanced CKD, stopping RAS inhibition was associated with higher absolute risks of mortality and major adverse cardiovascular events, but also with a lower absolute risk of initiating KRT.
在患有晚期 CKD 的患者中停止肾素-血管紧张素系统(RAS)抑制剂治疗是否会影响结局尚不清楚。
我们研究了在 2007 年至 2017 年期间在瑞典肾脏登记处登记并接受肾科医生治疗的患者,这些患者在接受 RAS 抑制剂治疗期间发展为晚期 CKD(eGFR<30 ml/min/1.73 m)。我们基于克隆、删失和加权使用目标试验模拟技术,比较了在 6 个月内停药和继续治疗与继续 RAS 抑制剂治疗的风险。这些风险包括随后 5 年全因死亡率、主要不良心血管事件和开始肾脏替代治疗(KRT)的风险。
在 10254 例新发生 eGFR<30 ml/min/1.73 m 的接受 RAS 抑制剂治疗的患者中,有 1553 例(15%)在 6 个月内停止 RAS 抑制剂治疗。中位 eGFR 为 23 ml/min/1.73 m。与继续 RAS 抑制相比,停止该治疗与更高的绝对 5 年死亡风险(40.9% vs 54.5%)和主要不良心血管事件风险(47.6% vs 59.5%)相关,但 KRT 风险较低(36.1% vs 27.9%);这相当于每 100 例患者中分别发生 13.6 例、11.9 例和 -8.3 例事件的绝对风险差异。这些结果在较高或较低 eGFR 时、在预先指定的亚组中、在调整白蛋白尿和钾水平并分层以及使用边缘结构模型将 RAS 抑制建模为时间依赖性暴露后、在整个研究中都是一致的。
在这项针对晚期 CKD 患者的全国性观察性研究中,停止 RAS 抑制与更高的绝对死亡和主要不良心血管事件风险相关,但也与较低的开始 KRT 的绝对风险相关。