Department of Pediatrics, Division of Pediatric Neurology, Kaohsiung Chang Gung Memorial Hospital, Chang Gung University College of Medicine, Kaohsiung 833, Taiwan.
Department of Pediatrics, Division of Genetics and Endocrinology, Linkou Chang Gung Memorial Hospital, Chang Gung University College of Medicine, Taoyan 333, Taiwan.
Nutrients. 2020 Dec 23;13(1):21. doi: 10.3390/nu13010021.
This study aimed to identify metabolic parameters at different time points of ketogenic diet therapy (KDT) and investigate their association with response to KDT in pediatric drug-resistant epilepsy (DRE).
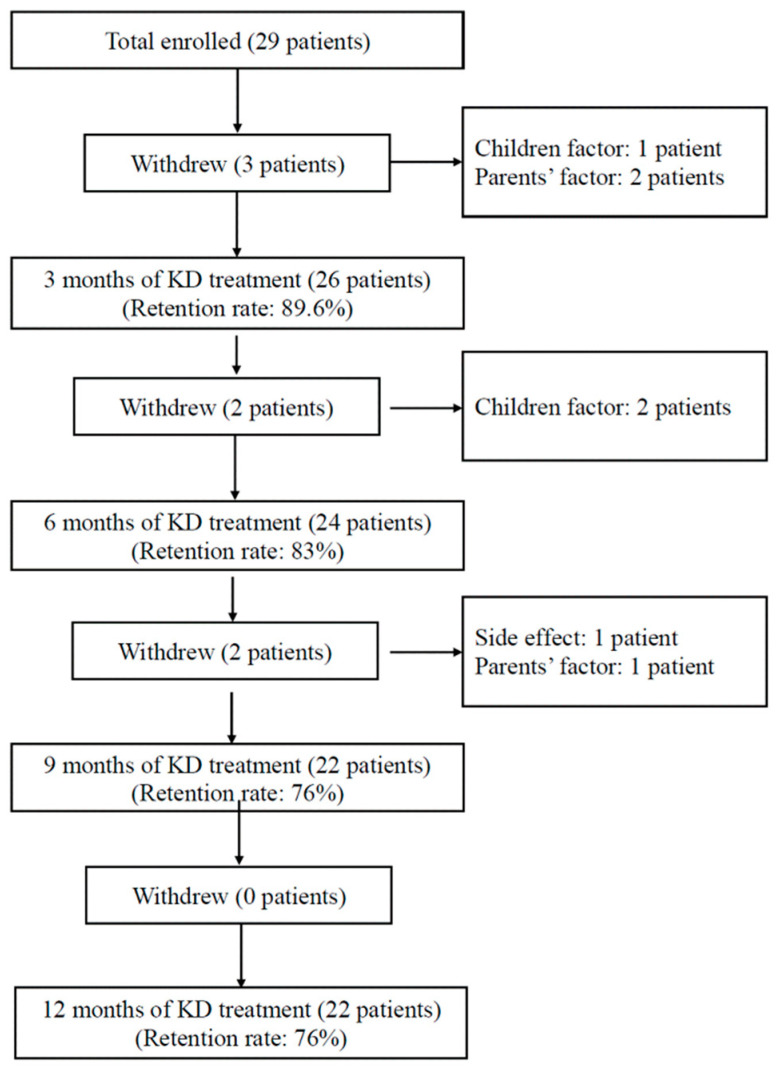
Prospectively, twenty-nine patients (0.67~20 years old) with DRE received classic ketogenic diet with non-fasting, gradual KD initiation protocol (GRAD-KD) for 1 year were enrolled. A total of 22 patients remaining in study received blood examinations at baseline, 3rd, 6th, 9th, and 12th months of KDT. β-hydroxybutyrate, free carnitine, acylcarnitines, and amino acids were compared between responders (seizure reduction rate ≥ 50%) and non-responders (seizure reduction rate < 50%) to identify the effectiveness of KDT.
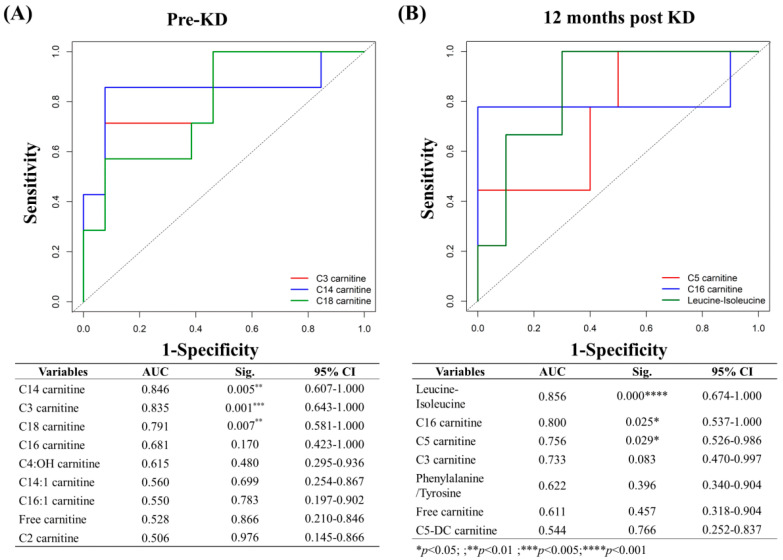
The 12-month retention rate was 76%. The responders after 12 months of KDT were 59% (13/22). The free carnitine level decreased significantly at 9th months ( < 0.001) but increased toward baseline without symptoms. Propionyl carnitine (C3), Isovaleryl carnitine (C5), 3-Hydroxyisovalerylcarnitine (C5:OH) and methylmalonyl carnitine (C4-DC) decreased but 3-hydroxybutyrylcarnitine (C4:OH) increased significantly at 12th months of KDT. The glycine level was persistently higher than baseline after KDT. KDT responders had lower baseline C3 and long-chain acylcarnitines, C14 and C18, as well as lower C5, C18, and leucine/isoleucine.
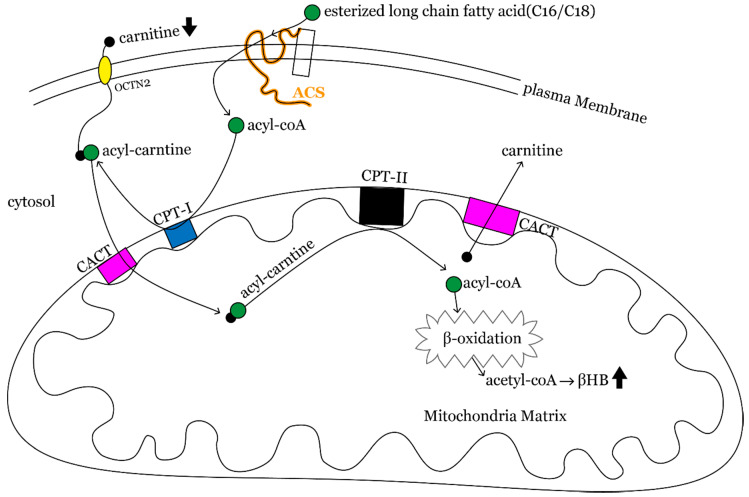
KDT should be avoided in patients with non-ketotic hyperglycemia. Routine carnitine supplementation is not recommended because hypocarnitinemia was transient and asymptomatic during KDT. Better mitochondrial βoxidation function associates with greater KDT response.
本研究旨在确定生酮饮食治疗(KDT)不同时间点的代谢参数,并探讨其与儿科耐药性癫痫(DRE)对 KDT 反应的关系。
前瞻性地,29 例 DRE 患者(0.67~20 岁)接受非禁食经典生酮饮食,采用逐步 KD 起始方案(GRAD-KD)治疗 1 年。共有 22 例患者在研究中接受了基线、第 3、6、9 和 12 个月的 KDT 血液检查。比较反应者(癫痫发作减少率≥50%)和非反应者(癫痫发作减少率<50%)的β-羟丁酸、游离肉碱、酰基肉碱和氨基酸,以确定 KDT 的有效性。
12 个月的保留率为 76%。KDT 治疗 12 个月后的反应者为 59%(13/22)。游离肉碱水平在第 9 个月显著下降(<0.001),但无症状地向基线回升。丙酰肉碱(C3)、异戊酰肉碱(C5)、3-羟基异戊酰肉碱(C5:OH)和甲基丙二酰肉碱(C4-DC)在 KDT 治疗 12 个月时降低,但 3-羟丁酸肉碱(C4:OH)显著升高。KDT 后甘氨酸水平持续高于基线。KDT 反应者的基线 C3 和长链酰基肉碱 C14 和 C18 较低,以及 C5、C18 和亮氨酸/异亮氨酸较低。
非酮性高血糖患者应避免进行 KDT。不建议常规补充肉碱,因为在 KDT 期间低肉碱血症是短暂的且无症状。更好的线粒体β氧化功能与更大的 KDT 反应相关。