Dahir Shukri, Cotache-Condor Cesia F, Concepcion Tessa, Mohamed Mubarak, Poenaru Dan, Adan Ismail Edna, Leather Andy J M, Rice Henry E, Smith Emily R
Edna Adan University Hospital, Hargeisa, Somaliland.
Department of Public Health, Baylor University, Waco, Texas, USA.
BMJ Open. 2020 Dec 29;10(12):e042968. doi: 10.1136/bmjopen-2020-042968.
The unmet burden of surgical care is high in low-income and middle-income countries. The Lancet Commission on Global Surgery (LCoGS) proposed six indicators to guide the development of national plans for improving and monitoring access to essential surgical care. This study aimed to characterise the Somaliland surgical health system according to the LCoGS indicators and provide recommendations for next-step interventions.
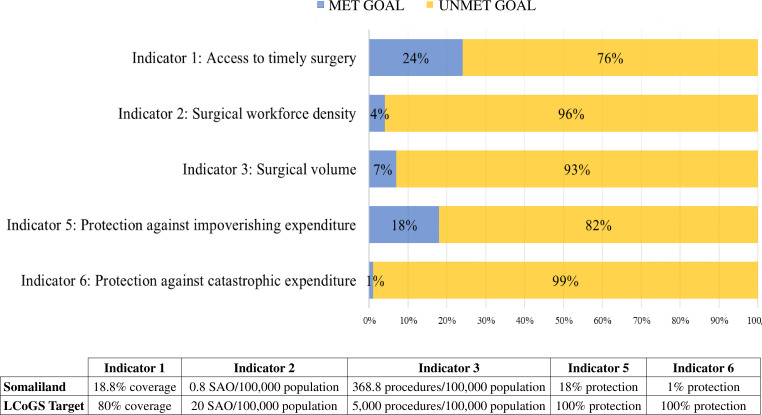
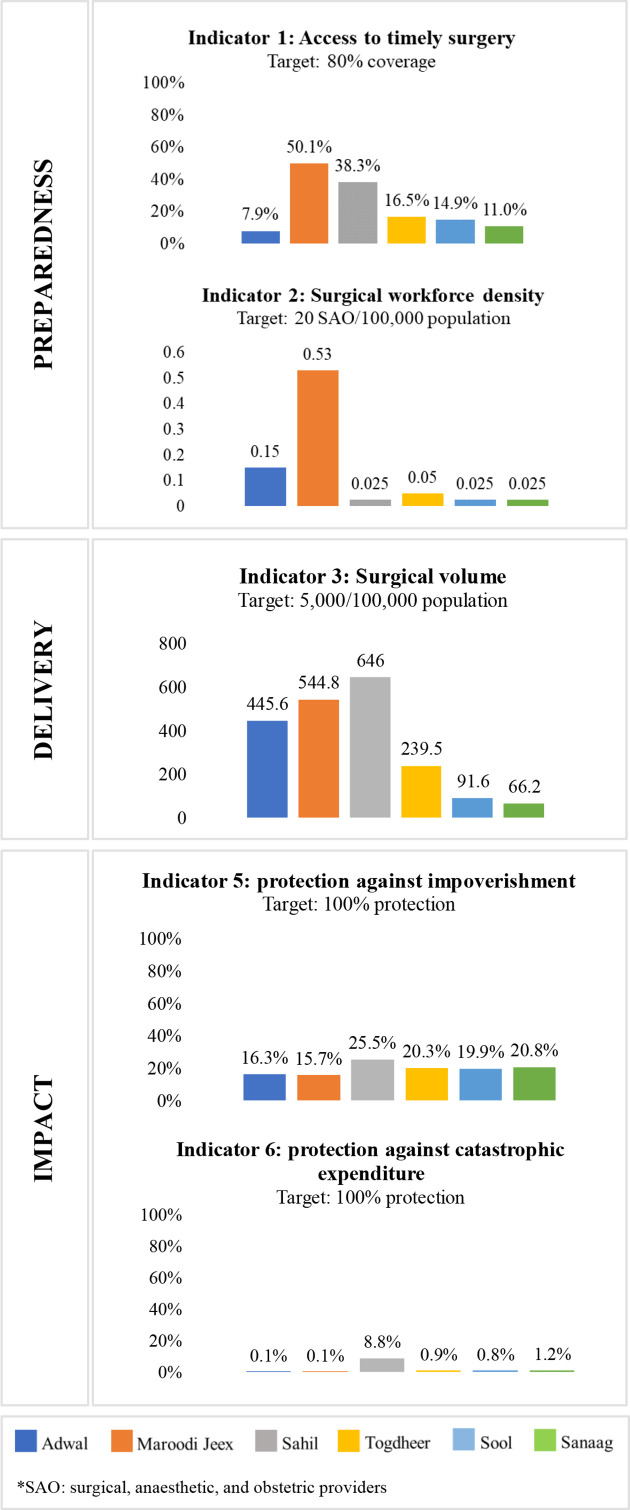
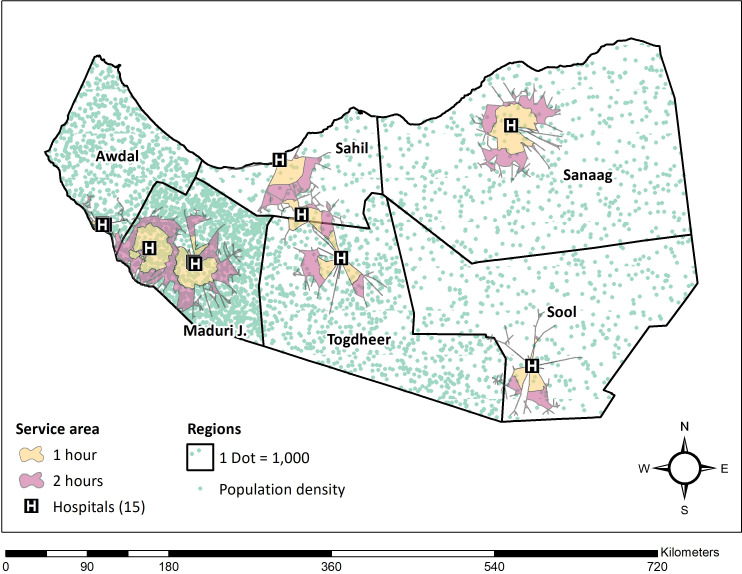
In this cross-sectional nationwide study, the WHO's Surgical Assessment Tool-Hospital Walkthrough and geographical mapping were used for data collection at 15 surgically capable hospitals. LCoGS indicators for was defined as access to timely surgery and specialist surgical workforce density (surgeons, anaesthesiologists and obstetricians/SAO), was defined as surgical volume, and was defined as protection against impoverishment and catastrophic expenditure. Indicators were compared with the LCoGS goals and were stratified by region.
The healthcare system in Somaliland does not meet any of the six LCoGS targets for preparedness, delivery or impact. We estimate that only 19% of the population has timely access to essential surgery, less than the LCoGS goal of 80% coverage. The number of specialist SAO providers is 0.8 per 100 000, compared with an LCoGS goal of 20 SAO per 100 000. Surgical volume is 368 procedures per 100 000 people, while the LCoGS goal is 5000 procedures per 100 000. Protection against impoverishing expenditures was only 18% and against catastrophic expenditures 1%, both far below the LCoGS goal of 100% protection.
We found several gaps in the surgical system in Somaliland using the LCoGS indicators and target goals. These metrics provide a broad view of current status and gaps in surgical care, and can be used as benchmarks of progress towards universal health coverage for the provision of safe, affordable, and timely surgical, obstetric and anaesthesia care in Somaliland.
在低收入和中等收入国家,外科护理未得到满足的负担很高。《柳叶刀》全球外科委员会(LCoGS)提出了六项指标,以指导制定改善和监测基本外科护理可及性的国家计划。本研究旨在根据LCoGS指标描述索马里兰外科卫生系统的特征,并为下一步干预措施提供建议。
在这项全国性横断面研究中,使用世界卫生组织的外科评估工具——医院巡查和地理绘图,在15家具备手术能力的医院收集数据。LCoGS指标中,指标1定义为及时手术的可及性和专科外科劳动力密度(外科医生、麻醉师和产科医生/SAO),指标2定义为手术量,指标3定义为防止贫困和灾难性支出。将指标与LCoGS目标进行比较,并按地区分层。
索马里兰的医疗系统在准备、提供或影响方面均未达到LCoGS的六项指标中的任何一项。我们估计,只有19%的人口能够及时获得基本手术,低于LCoGS覆盖80%的目标。专科SAO提供者的数量为每10万人0.8人,而LCoGS的目标是每10万人20名SAO。手术量为每10万人368例手术,而LCoGS的目标是每10万人5000例。防止贫困支出的比例仅为18%,防止灾难性支出的比例为1%,均远低于LCoGS 100%保护的目标。
我们使用LCoGS指标和目标发现了索马里兰外科系统中的几个差距。这些指标提供了外科护理当前状况和差距的广泛视图,并可作为索马里兰实现全民健康覆盖以提供安全、可负担和及时的外科、产科和麻醉护理的进展基准。