Department of Internal Medicine, San Cecilio University Hospital, Hospital Universitario San Cecilio, Avda. del Conocimiento s/n, 18016, Granada, Spain.
Department of Rheumatology, San Cecilio University Hospital, Granada, Spain.
Intern Emerg Med. 2021 Jun;16(4):843-852. doi: 10.1007/s11739-020-02600-z. Epub 2021 Jan 5.
Little evidence appears to exist for the use of anakinra, a recombinant interleukin-1 receptor antagonist, after non-response to treatment with corticosteroids alone or combined with tocilizumab in patients with severe COVID-19 pneumonia and moderate hyperinflammatory state.
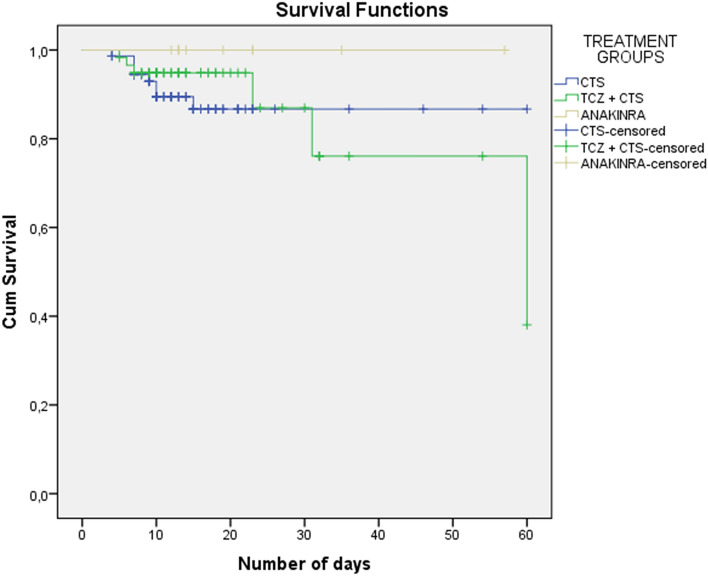
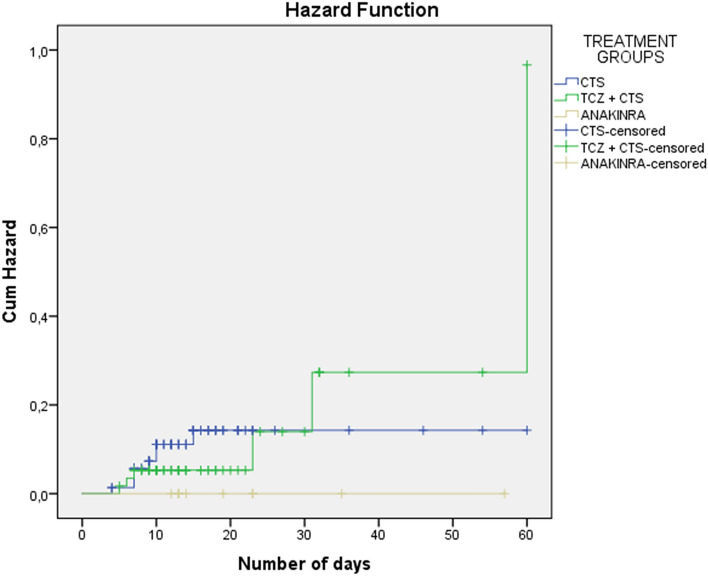
A retrospective observational cohort study was carried out involving 143 patients with severe COVID-19 pneumonia and moderate hyperinflammation. They received standard therapy along with pulses of methylprednisolone (group 1) or methylprednisolone plus tocilizumab (group 2), with the possibility of receiving anakinra (group 3) according to protocol. The aim of this study was to assess the role of anakinra in the clinical course (death, admission to the intensive care ward) during the first 60 days after the first corticosteroid pulse. Clinical, laboratory, and imaging characteristics as well as infectious complications were also analyzed.
74 patients (51.7%) in group 1, 59 (41.3%) patients in group 2, and 10 patients (7%) in group 3 were included. 8 patients (10.8%) in group 1 died, 6 (10.2%) in group 2, and 0 (0%) in group 3. After adjustment for age and clinical severity indices, treatment with anakinra was associated with a reduced risk of mortality (adjusted hazard ratio 0.518, 95% CI 0.265-0.910; p = 0.0437). Patients in group 3 had a lower mean CD4 count after 3 days of treatment. No patients in this group presented infectious complications.
In patients with moderate hyperinflammatory state associated with severe COVID-19 pneumonia, treatment with anakinra after non-response to corticosteroids or corticosteroids plus tocilizumab therapy may be an option for the management of these patients and may improve their prognosis.
对于 COVID-19 重症肺炎伴中度炎症反应综合征的患者,在单独使用或联合使用糖皮质激素及托珠单抗治疗后无反应,此时使用阿那白滞素(一种重组白细胞介素-1 受体拮抗剂)的证据似乎很少。
本研究回顾性观察了 143 例 COVID-19 重症肺炎伴中度炎症反应综合征患者,所有患者均接受标准治疗,联合使用甲泼尼龙冲击治疗(第 1 组)或甲泼尼龙联合托珠单抗(第 2 组),根据方案可能会使用阿那白滞素(第 3 组)。本研究旨在评估阿那白滞素在首次使用糖皮质激素后 60 天内对临床转归(死亡、入住重症监护病房)的影响。还分析了临床、实验室和影像学特征以及感染并发症。
第 1 组 74 例(51.7%),第 2 组 59 例(41.3%),第 3 组 10 例(7%)。第 1 组有 8 例(10.8%)死亡,第 2 组有 6 例(10.2%)死亡,第 3 组无死亡病例。校正年龄和临床严重程度指数后,阿那白滞素治疗与降低死亡率相关(调整后的危险比为 0.518,95%CI 0.265-0.910;p=0.0437)。第 3 组患者在治疗 3 天后的平均 CD4 计数较低。该组无患者出现感染并发症。
对于 COVID-19 重症肺炎伴中度炎症反应综合征的患者,在糖皮质激素或糖皮质激素联合托珠单抗治疗无反应后使用阿那白滞素可能是治疗这些患者的一种选择,并可能改善其预后。