Toor Kabirraaj, Middleton Mark R, Chan Keith, Amadi Adenike, Moshyk Andriy, Kotapati Srividya
Precision HEOR, 1505 West 2nd Avenue, Vancouver, BC, V6H 3Y4, Canada.
University of Oxford, Old Road Campus Research Building, Roosevelt Drive, Oxford, OX3 7DQ, UK.
BMC Cancer. 2021 Jan 5;21(1):3. doi: 10.1186/s12885-020-07538-1.
Immune checkpoint inhibitors and targeted therapies are approved for adjuvant treatment of patients with resected melanoma; however, they have not been compared in randomized controlled trials (RCTs). We compared the efficacy and safety of adjuvant nivolumab with other approved treatments using available evidence from RCTs in a Bayesian network meta-analysis (NMA).
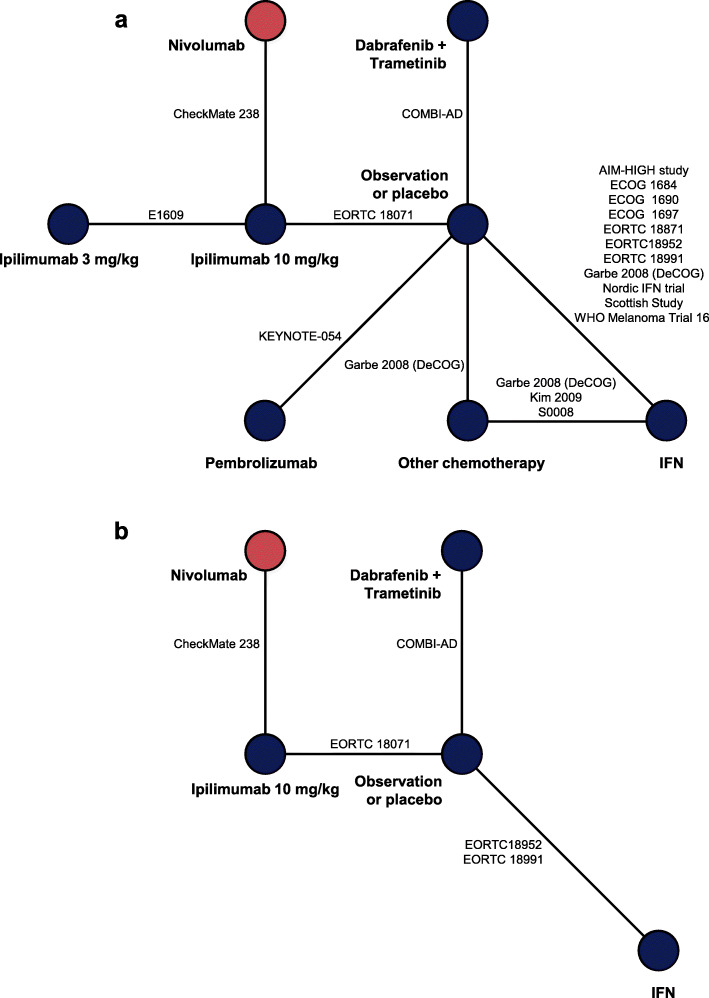
A systematic literature review was conducted through May 2019 to identify relevant RCTs evaluating approved adjuvant treatments. Outcomes of interest included recurrence-free survival (RFS)/disease-free survival (DFS), distant metastasis-free survival (DMFS), all-cause grade 3/4 adverse events (AEs), discontinuations, and discontinuations due to AEs. Time-to-event outcomes (RFS/DFS and DMFS) were analyzed both assuming that hazard ratios (HRs) are constant over time and that they vary.
Of 26 identified RCTs, 19 were included in the NMA following a feasibility assessment. Based on HRs for RFS/DFS, the risk of recurrence with nivolumab was similar to that of pembrolizumab and lower than that of ipilimumab 3 mg/kg, ipilimumab 10 mg/kg, or interferon. Risk of recurrence with nivolumab was similar to that of dabrafenib plus trametinib at 12 months, however, was lower beyond 12 months (HR [95% credible interval] at 24 months, 0.46 [0.27-0.78]; at 36 months, 0.28 [0.14-0.59]). Based on HRs for DMFS, the risk of developing distant metastases was lower with nivolumab than with ipilimumab 10 mg/kg or interferon and was similar to dabrafenib plus trametinib.
Adjuvant therapy with nivolumab provides an effective treatment option with a promising risk-benefit profile.
免疫检查点抑制剂和靶向治疗已被批准用于黑色素瘤切除患者的辅助治疗;然而,它们尚未在随机对照试验(RCT)中进行比较。我们在一项贝叶斯网络荟萃分析(NMA)中,利用RCT的现有证据比较了辅助性纳武利尤单抗与其他已批准治疗方法的疗效和安全性。
进行了一项系统的文献综述,截至2019年5月,以确定评估已批准辅助治疗的相关RCT。感兴趣的结果包括无复发生存期(RFS)/无病生存期(DFS)、无远处转移生存期(DMFS)、全因3/4级不良事件(AE)、停药以及因AE导致的停药。对事件发生时间的结果(RFS/DFS和DMFS)进行了分析,分析时既假设风险比(HR)随时间恒定,也假设其随时间变化。
在确定的26项RCT中,经过可行性评估后,19项被纳入NMA。基于RFS/DFS的HR,纳武利尤单抗的复发风险与帕博利珠单抗相似,低于3mg/kg伊匹木单抗、10mg/kg伊匹木单抗或干扰素。纳武利尤单抗在12个月时的复发风险与达拉非尼加曲美替尼相似,但在12个月后较低(24个月时的HR[95%可信区间]为0.46[0.27 - 0.78];36个月时为0.28[0.14 - 0.59])。基于DMFS的HR,纳武利尤单抗发生远处转移的风险低于10mg/kg伊匹木单抗或干扰素,与达拉非尼加曲美替尼相似。
纳武利尤单抗辅助治疗提供了一种有效的治疗选择,具有良好的风险效益比。