Saoraya Jutamas, Wongsamita Lipda, Srisawat Nattachai, Musikatavorn Khrongwong
Division of Academic Affairs, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand.
Department of Emergency Medicine, King Chulalongkorn Memorial Hospital, The Thai Red Cross Society, 1873 Rama IV Road, Pathumwan, Bangkok, 10330, Thailand.
J Intensive Care. 2021 Jan 5;9(1):1. doi: 10.1186/s40560-020-00515-7.
Aggressive fluid administration is recommended in the resuscitation of septic patients. However, the delivery of a rapid fluid bolus might cause harm by inducing degradation of the endothelial glycocalyx. This research aimed to examine the effects of the limited infusion rate of fluid on glycocalyx shedding as measured by syndecan-1 in patients with sepsis-induced hypoperfusion.
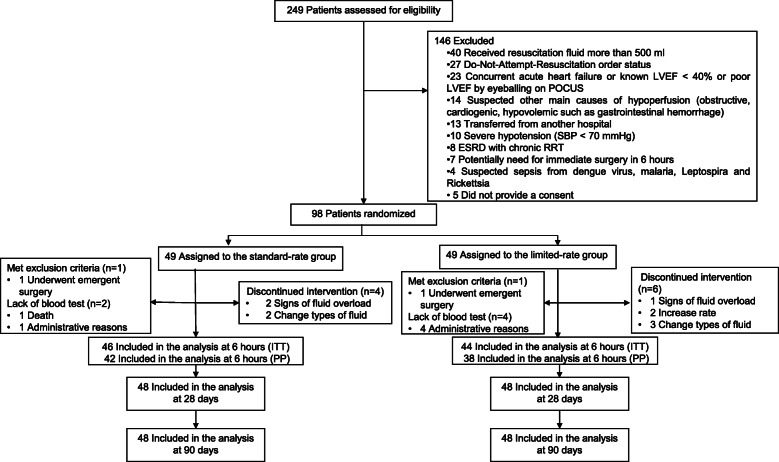
A prospective, randomized, controlled, open-label trial was conducted between November 2018 and February 2020 in an urban academic emergency department. Patients with sepsis-induced hypoperfusion, defined as hypotension or hyperlactatemia, were randomized to receive either the standard rate (30 ml/kg/h) or limited rate (10 ml/kg/h) of fluid for the first 30 ml/kg fluid resuscitation. Subsequently, the fluid rate was adjusted according to the physician's discretion but not more than that of the designated fluid rate for the total of 6 h. The primary outcome was differences in change of syndecan-1 levels at 6 h compared to baseline between standard and limited rate groups. Secondary outcomes included adverse events, organ failure, and 90-day mortality.
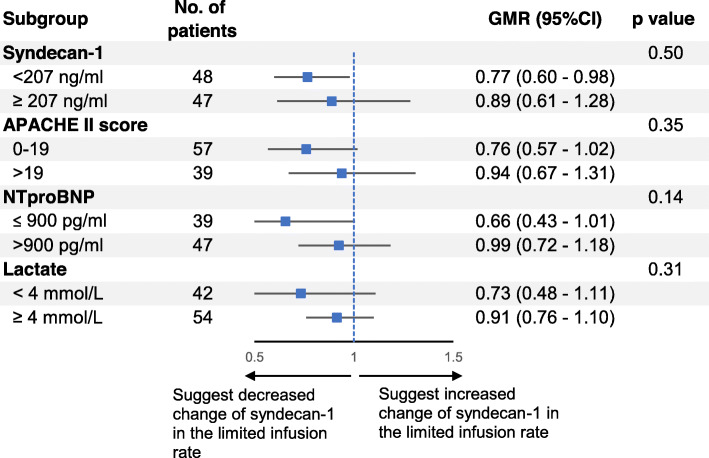
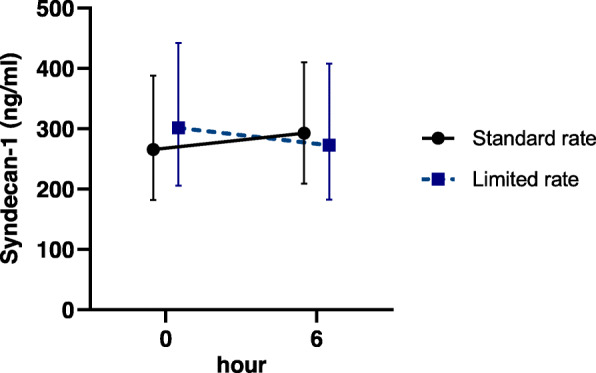
We included 96 patients in the intention-to-treat analysis, with 48 assigned to the standard-rate strategy and 48 to the limited-rate strategy. The median fluid volume in 6 h in the limited-rate group was 39 ml/kg (interquartile range [IQR] 35-52 ml/kg) vs. 53 ml/kg (IQR 46-64 ml/kg) in the standard-rate group (p < 0.001). Patients in the limited-rate group were less likely to received vasopressors (17% vs 42%; p = 0.007) and mechanical ventilation (20% vs 41%; p = 0.049) during the first 6 h. There were no significantly different changes in syndecan-1 levels at 6 h between the two groups (geometric mean ratio [GMR] in the limited-rate group, 0.82; 95% confidence interval [CI], 0.66-1.02; p = 0.07). There were no significant differences in adverse events, organ failure outcomes, or mortality between the two groups.
In sepsis resuscitation, the limited rate of fluid resuscitation compared to the standard rate did not significantly reduce changes in syndecan-1 at 6 h.
Thai Clinical Trials Registry number: TCTR20181010001. Registered 8 October 2018, http://www.clinicaltrials.in.th/index.php?tp=regtrials&menu=trialsearch&smenu=fulltext&task=search&task2=view1&id=4064.
对于脓毒症患者的复苏,建议积极进行液体输注。然而,快速推注液体可能会因诱导内皮糖萼降解而造成损害。本研究旨在探讨在脓毒症诱导的低灌注患者中,有限的输液速率对通过syndecan-1测量的糖萼脱落的影响。
2018年11月至2020年2月在一家城市学术急诊科进行了一项前瞻性、随机、对照、开放标签试验。脓毒症诱导的低灌注患者(定义为低血压或高乳酸血症)被随机分配在最初30 ml/kg液体复苏时接受标准速率(30 ml/kg/h)或有限速率(10 ml/kg/h)的液体。随后,根据医生的判断调整输液速率,但在总共6小时内不超过指定的输液速率。主要结局是标准速率组和有限速率组在6小时时与基线相比syndecan-1水平变化的差异。次要结局包括不良事件、器官衰竭和90天死亡率。
在意向性分析中,我们纳入了96例患者,48例被分配到标准速率策略组,48例被分配到有限速率策略组。有限速率组6小时内的液体量中位数为39 ml/kg(四分位间距[IQR] 35 - 52 ml/kg),而标准速率组为53 ml/kg(IQR 46 - 64 ml/kg)(p < 0.001)。有限速率组的患者在最初6小时内接受血管加压药治疗的可能性较小(17%对42%;p = 0.)和机械通气的可能性较小(20%对41%;p = 0.049)。两组在6小时时syndecan-1水平的变化无显著差异(有限速率组的几何平均比[GMR]为0.82;95%置信区间[CI],0.66 - 1.02;p = 0.07)。两组在不良事件、器官衰竭结局或死亡率方面无显著差异。
在脓毒症复苏中,与标准速率相比,有限的液体复苏速率在6小时时并未显著降低syndecan-1的变化。
泰国临床试验注册号:TCTR20181010001。于2018年10月8日注册,http://www.clinicaltrials.in.th/index.php?tp=regtrials&menu=trialsearch&smenu=fulltext&task=search&task2=view1&id=4064。