Division of Pulmonary and Critical Care Medicine, Department of Medicine, Mayo Clinic, 200 First Street SW, Rochester, MN, 55905, USA.
Department of Critical Care Medicine, Zhongnan Hospital of Wuhan University, 169 East Lake Road, PO Box 430071, Wuhan, Hubei, China.
Crit Care. 2020 Apr 7;24(1):137. doi: 10.1186/s13054-020-2819-5.
Fluid resuscitation has become the cornerstone of early septic shock management, but the optimal fluid rate is still not well studied. The goal of this investigation is to examine the relationship between fluid resuscitation rate and septic shock resolution.
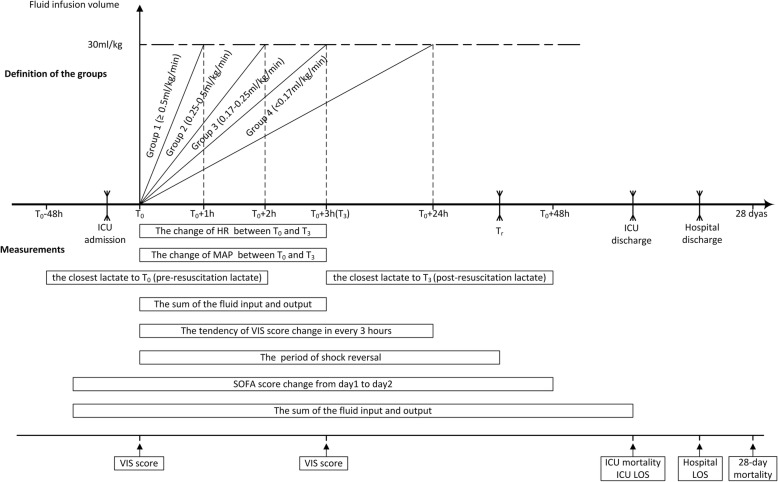
We retrospectively studied adult (≥ 18 years) patients with septic shock, defined based on sepsis III definition, from January 1, 2006, through May 31, 2018, in the medical intensive care unit (MICU) of Mayo Clinic Rochester. The fluid resuscitation time was defined as the time required to infuse the initial fluid bolus of 30 ml/kg, based on the recommendations of the 2016 surviving sepsis campaign. The cohort was divided into four groups based on the average fluid rate (group 1 ≥ 0.5, group 2 0.25-0.49, group 3 0.17-0.24, and group 4 < 0.17 ml/kg/min). The primary outcome was the time to shock reversal. Multivariable regression analyses were conducted to account for potential confounders.
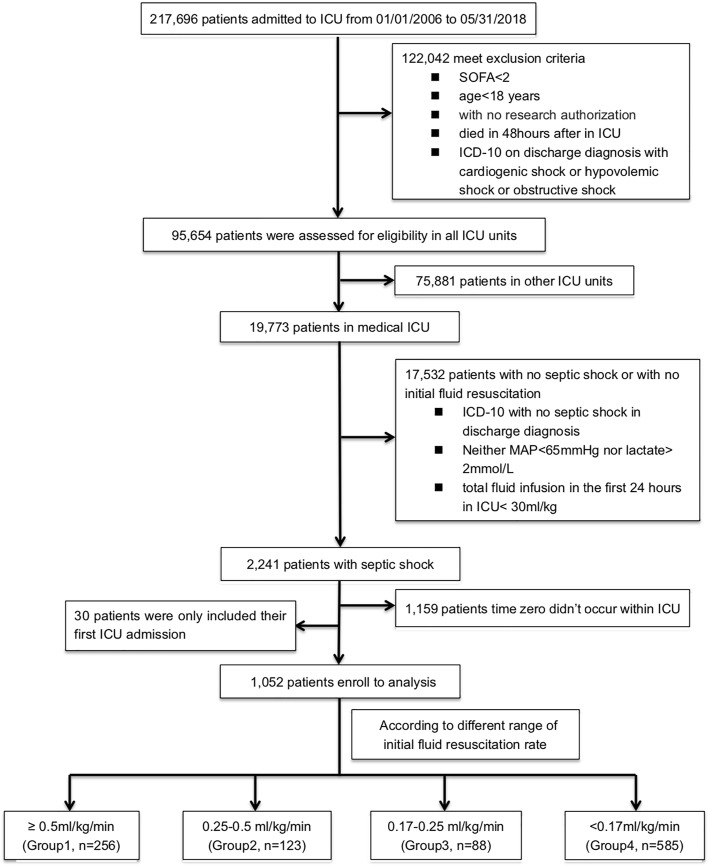
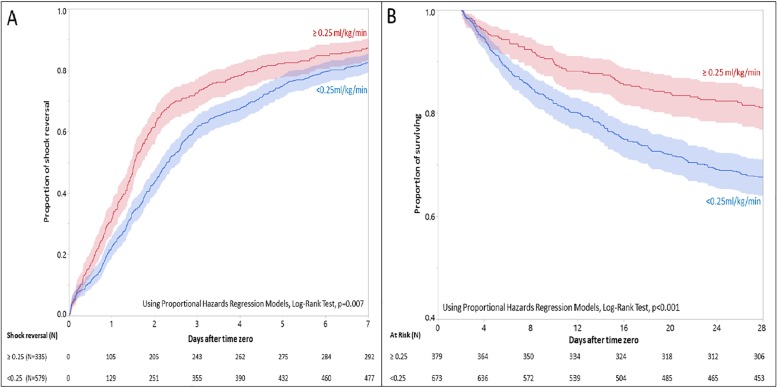
A total of 1052 patients met eligibility criteria and were included in the analysis. The time-to-shock reversal was significantly different among the groups (P < .001). Patients in group 1 who received fluid resuscitation at a faster rate had a shorter time to shock reversal (HR = 0.78; 95% CI 0.66-0.91; P = .01) when compared with group 4 with a median (IQR) time-to-shock reversal of 1.7 (1.5, 2.0) vs. 2.8 (2.6, 3.3) days, respectively. Using 0.25 ml/kg/min as cutoff, the higher fluid infusion rate was associated with a shorter time to shock reversal (HR = 1.22; 95% CI 1.06-1.41; P = .004) and with decreased odds of 28-day mortality (HR = 0.71; 95% CI 0.60-0.85; P < .001).
In septic shock patients, initial fluid resuscitation rate of 0.25-0.50 ml/kg/min (i.e., completion of the initial 30 ml/kg IV fluid resuscitation within the first 2 h), may be associated with early shock reversal and lower 28-day mortality compared with slower rates of infusion.
液体复苏已成为治疗早期感染性休克的基石,但最佳液体量仍未得到充分研究。本研究旨在探讨液体复苏率与感染性休克缓解的关系。
我们回顾性研究了 2006 年 1 月 1 日至 2018 年 5 月 31 日期间 Mayo 诊所罗彻斯特医学重症监护病房(MICU)中基于败血症 III 定义的成年(≥18 岁)感染性休克患者。根据 2016 年拯救败血症运动的建议,将液体复苏时间定义为输注初始 30ml/kg 液体冲击量所需的时间。根据平均液体速度将队列分为四组(组 1 ≥0.5,组 2 0.25-0.49,组 3 0.17-0.24,组 4 <0.17ml/kg/min)。主要结局是休克逆转时间。进行多变量回归分析以考虑潜在的混杂因素。
共有 1052 名符合入选标准的患者纳入分析。组间休克逆转时间差异有统计学意义(P<0.001)。与组 4 相比,以更快速度接受液体复苏的组 1 患者休克逆转时间更短(HR=0.78;95%CI 0.66-0.91;P=0.01),组 1 患者休克逆转的中位数(IQR)时间为 1.7(1.5,2.0)天,组 4 为 2.8(2.6,3.3)天。以 0.25ml/kg/min 为截断值,较高的液体输注速度与休克逆转时间更短相关(HR=1.22;95%CI 1.06-1.41;P=0.004),28 天死亡率降低(HR=0.71;95%CI 0.60-0.85;P<0.001)。
在感染性休克患者中,与较慢的输注速度相比,初始液体复苏率为 0.25-0.50ml/kg/min(即,在最初 2 小时内完成初始 30ml/kg 静脉液体复苏),可能与早期休克逆转和较低的 28 天死亡率相关。