Department of Gastroenterology and Metabolism, Nagoya City University Graduate School of Medical Sciences, Nagoya, Japan.
Gut Liver. 2021 May 15;15(3):476-485. doi: 10.5009/gnl20238.
BACKGROUND/AIMS: Although endoscopic transpapillary gallbladder drainage (ETGBD) has been reported as an alternative procedure for acute cholecystitis, it requires advanced endoscopic techniques. In terms of the certainty of achieving drainage, it remains a challenging procedure. The aim of the current study was to elucidate the practical efficacy of cholangioscopic assistance and to develop a new classification that could be used to evaluate the technical difficulty of ETGBD and provide a theoretical strategy to apply cholangioscopy appropriately for difficult ETGBD.
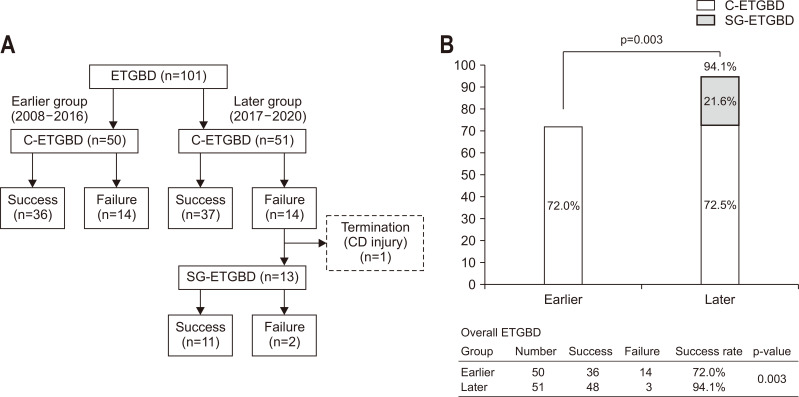
A total of 101 patients undergoing ETGBD were retrospectively studied. The characteristics and technical outcomes of ETGBD with conventional ETGBD (C-ETGBD) and SpyGlass DS-assisted ETGBD (SG-ETGBD) were evaluated. The characteristics and technique-dependent factors of unsuccessful C-ETGBD/SG-ETGBD were evaluated using the classification based on the steps of the procedure. The predictive factors of successful C-ETGBD/SG-ETGBD were examined.
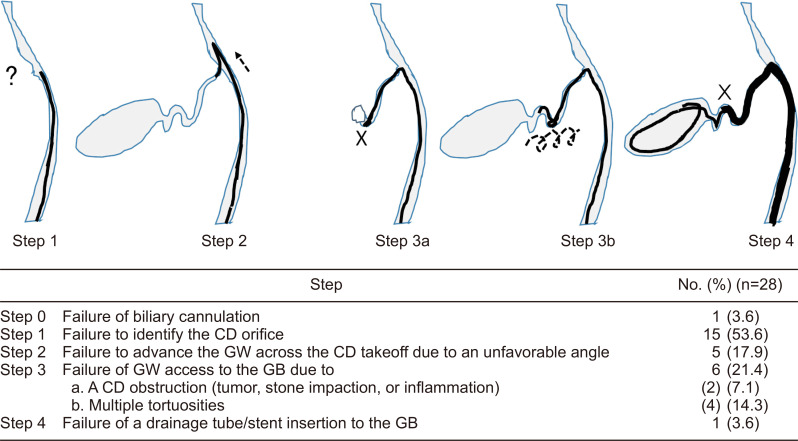
C-ETGBD was successful in 73 patients (72.3%). SG-ETGBD was successful in 11 of 13 patients (84.6%) who had C-ETGBD failure. Optional SG-ETGBD significantly increased the final success rate (94.1%) compared to C-ETGBD alone (p=0.003). ETGBD procedures could be classified into four steps. SG-assistance worked as an excellent troubleshooter in step 1 (failure to identify the cystic duct orifice) and step 2 (failure of guidewire advancement across the downturned angle of cystic duct takeoff). Magnetic resonance cholangiopancreatography could provide predictive information based on the classification.
Optional SG-ETGBD achieved a significantly higher success rate than C-ETGBD alone. Step classification is helpful for determining the technical difficulty of ETGBD and developing a theoretical strategy to apply cholangioscopy in a coordinated manner.
背景/目的:尽管经内镜经胆囊管引流术(ETGBD)已被报道为急性胆囊炎的一种替代治疗方法,但它需要先进的内镜技术。就实现引流的确定性而言,它仍然是一项具有挑战性的操作。本研究旨在阐明胆管镜辅助的实际疗效,并制定一种新的分类方法,用于评估 ETGBD 的技术难度,并提供一种理论策略,以便适当地应用胆管镜。
回顾性研究了 101 例行 ETGBD 的患者。评估了常规 ETGBD(C-ETGBD)和 SpyGlass DS 辅助 ETGBD(SG-ETGBD)的特点和技术结果。使用基于操作步骤的分类方法,评估了 C-ETGBD/SG-ETGBD 失败的特征和技术相关因素。检查了 C-ETGBD/SG-ETGBD 成功的预测因素。
73 例(72.3%)患者 C-ETGBD 成功。C-ETGBD 失败的 13 例患者中,11 例 SG-ETGBD 成功(84.6%)。与单独 C-ETGBD 相比,选择性 SG-ETGBD 显著提高了最终成功率(94.1%)(p=0.003)。ETGBD 操作可分为四个步骤。SG 辅助在步骤 1(未能识别胆囊管口)和步骤 2(导丝不能穿过胆囊管起始处的弯道)中表现出色。磁共振胰胆管造影术可根据分类提供预测信息。
选择性 SG-ETGBD 比单独 C-ETGBD 成功率显著提高。步骤分类有助于确定 ETGBD 的技术难度,并制定一种理论策略,以便协调地应用胆管镜。