Raat Willem, Smeets Miek, Janssens Stefan, Vaes Bert
Department of Public Health and Primary Care, KU Leuven (KUL), Kapucijnenvoer 33, Blok J Bus 7001, Leuven, 3000, Belgium.
Department of Cardiovascular Diseases, University Hospitals, KU Leuven (KUL), Leuven, Belgium.
ESC Heart Fail. 2021 Apr;8(2):802-818. doi: 10.1002/ehf2.13152. Epub 2021 Jan 6.
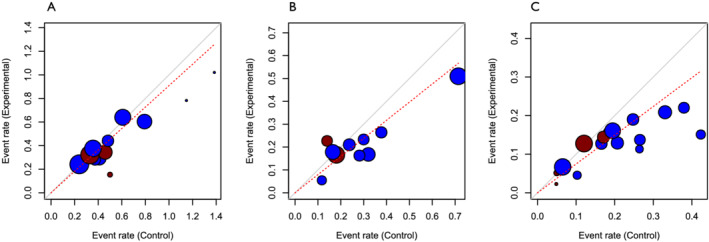
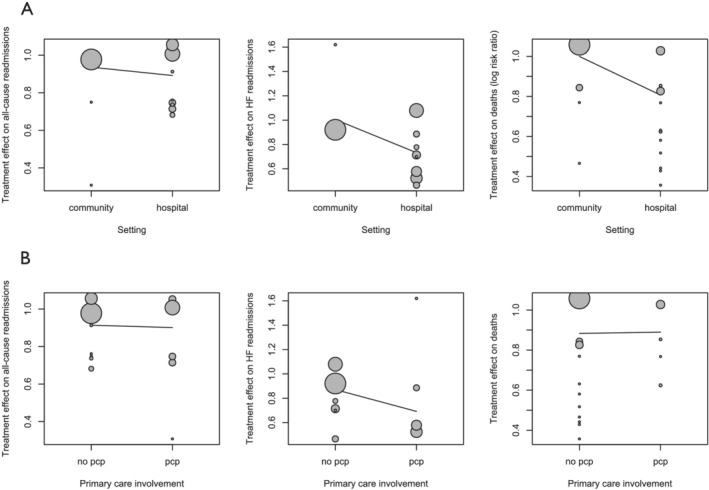
Multidisciplinary disease management programmes (DMPs) are a cornerstone of modern guideline-recommended care for heart failure (HF). Few programmes are community initiated or involve primary care professionals, despite the importance of home-based care for HF. We compared the outcomes of different multidisciplinary HF DMPs in relation to their recruitment setting and involvement of primary care health professionals. We conducted a systematic review and meta-analysis of randomized controlled trials published in MEDLINE, Embase, and Cochrane between 2000 and 2020 using Cochrane Collaboration methodology. Our meta-analysis included 19 randomized controlled trials (7577 patients), classified according to recruitment setting and involvement of primary care professionals. Thirteen studies recruited in the hospital (n = 5243 patients) and six in the community (n = 2334 patients). Only six studies involved primary care professionals (n = 3427 patients), with two of these recruited in the community (n = 225 patients). Multidisciplinary HF DMPs that recruited in the community had no significant effect on all-cause and HF readmissions nor on mortality, irrespective of primary care involvement. Studies that recruited in the hospital demonstrated a significant reduction in mortality (relative risk 0.87, 95% confidence interval [CI] [0.76, 0.98]), HF readmissions (0.70, 95% CI [0.54, 0.89]), and all-cause readmissions (0.72, 95% CI [0.60, 0.87]). However, the difference in effect size between recruitment setting and involvement of primary care was not significant in a meta-regression analysis. Multidisciplinary HF DMPs that recruit in the community have no significant effect on mortality or hospital readmissions, unlike DMPs that recruit in the hospital, although the difference in effect size was not significant in a meta-regression analysis. Only six multidisciplinary studies involved primary care professionals. Given demographic evolutions and the importance of integrated home-based care for patients with HF, future multidisciplinary HF DMPs should consider integrating primary care professionals and evaluating the effectiveness of this model.
多学科疾病管理项目(DMPs)是现代指南推荐的心力衰竭(HF)护理的基石。尽管居家护理对心力衰竭很重要,但很少有项目是由社区发起的,也很少有初级保健专业人员参与其中。我们比较了不同多学科心力衰竭DMPs在招募地点和初级保健卫生专业人员参与方面的结果。我们使用Cochrane协作方法,对2000年至2020年期间发表在MEDLINE、Embase和Cochrane上的随机对照试验进行了系统评价和荟萃分析。我们的荟萃分析包括19项随机对照试验(7577名患者),根据招募地点和初级保健专业人员的参与情况进行分类。13项研究在医院招募(n = 5243名患者),6项在社区招募(n = 2334名患者)。只有6项研究涉及初级保健专业人员(n = 3427名患者),其中2项在社区招募(n = 225名患者)。无论初级保健是否参与,在社区招募的多学科心力衰竭DMPs对全因再入院率、心力衰竭再入院率和死亡率均无显著影响。在医院招募的研究显示死亡率显著降低(相对风险0.87,95%置信区间[CI][0.76,0.98]),心力衰竭再入院率(0.70,95%CI[0.54,0.89])和全因再入院率(0.72,95%CI[0.60,0.87])。然而,在荟萃回归分析中,招募地点和初级保健参与之间的效应大小差异并不显著。与在医院招募的DMPs不同,在社区招募的多学科心力衰竭DMPs对死亡率或医院再入院率没有显著影响,尽管在荟萃回归分析中效应大小差异不显著。只有6项多学科研究涉及初级保健专业人员。考虑到人口结构的变化以及居家综合护理对心力衰竭患者的重要性,未来的多学科心力衰竭DMPs应考虑纳入初级保健专业人员并评估该模式的有效性。