Department of Epidemiology, Epidemiology, Biostatistics and Prevention Institute (EBPI), University of Zurich, Hirschengraben 84, 8001, Zurich, Switzerland.
Faculty of Medicine (MeF), University of Zurich, Pestalozzistrasse 3, 8091, Zurich, Switzerland.
Crit Care. 2021 Jan 6;25(1):16. doi: 10.1186/s13054-020-03446-9.
This systematic review and meta-analysis aimed to determine the effectiveness of systematic early mobilization in improving muscle strength and physical function in mechanically ventilated intensive care unit (ICU) patients.
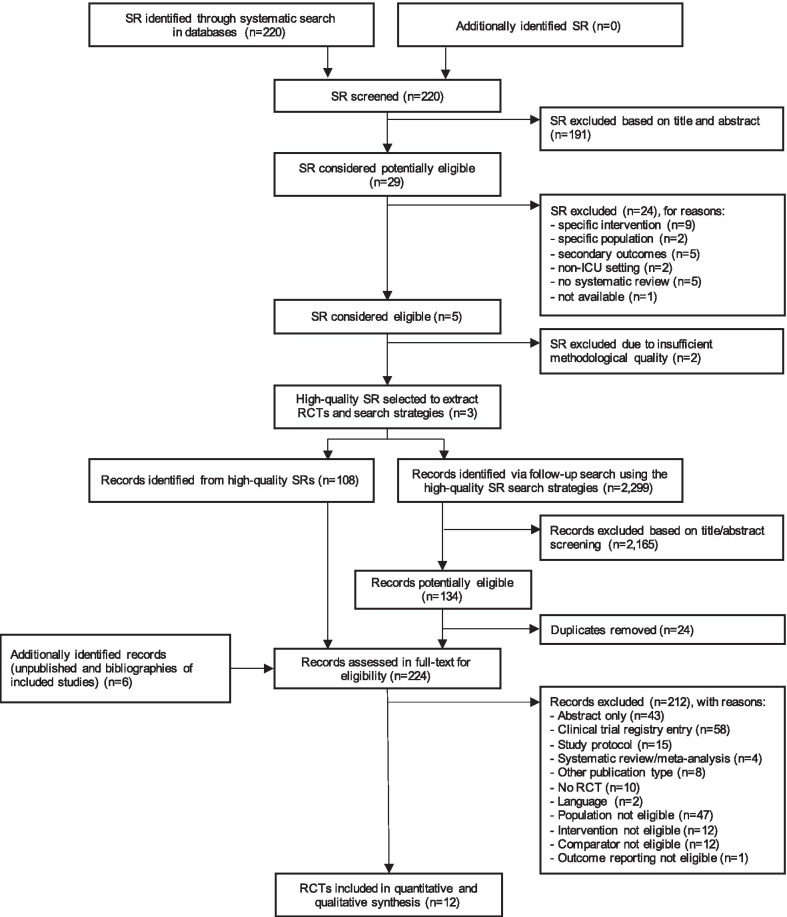
We conducted a two-stage systematic literature search in MEDLINE, EMBASE and the Cochrane Library until January 2019 for randomized controlled trials (RCTs) examining the effects of early mobilization initiated within 7 days after ICU admission compared with late mobilization, standard early mobilization or no mobilization. Priority outcomes were Medical Research Council Sum Score (MRC-SS), incidence of ICU-acquired weakness (ICUAW), 6-min walk test (6MWT), proportion of patients reaching independence, time needed until walking, SF-36 Physical Function Domain Score (PFS) and SF-36 Physical Health Component Score (PCS). Meta-analysis was conducted where sufficient comparable evidence was available. We evaluated the certainty of evidence according to the GRADE approach.
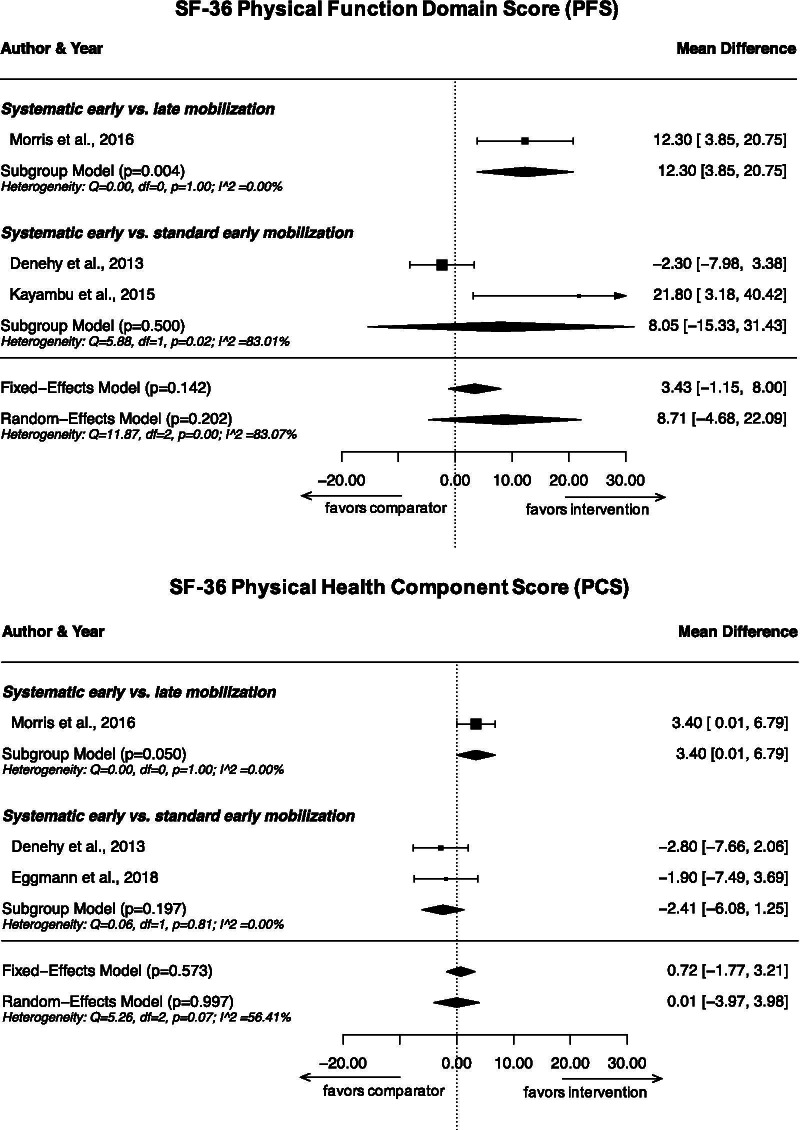
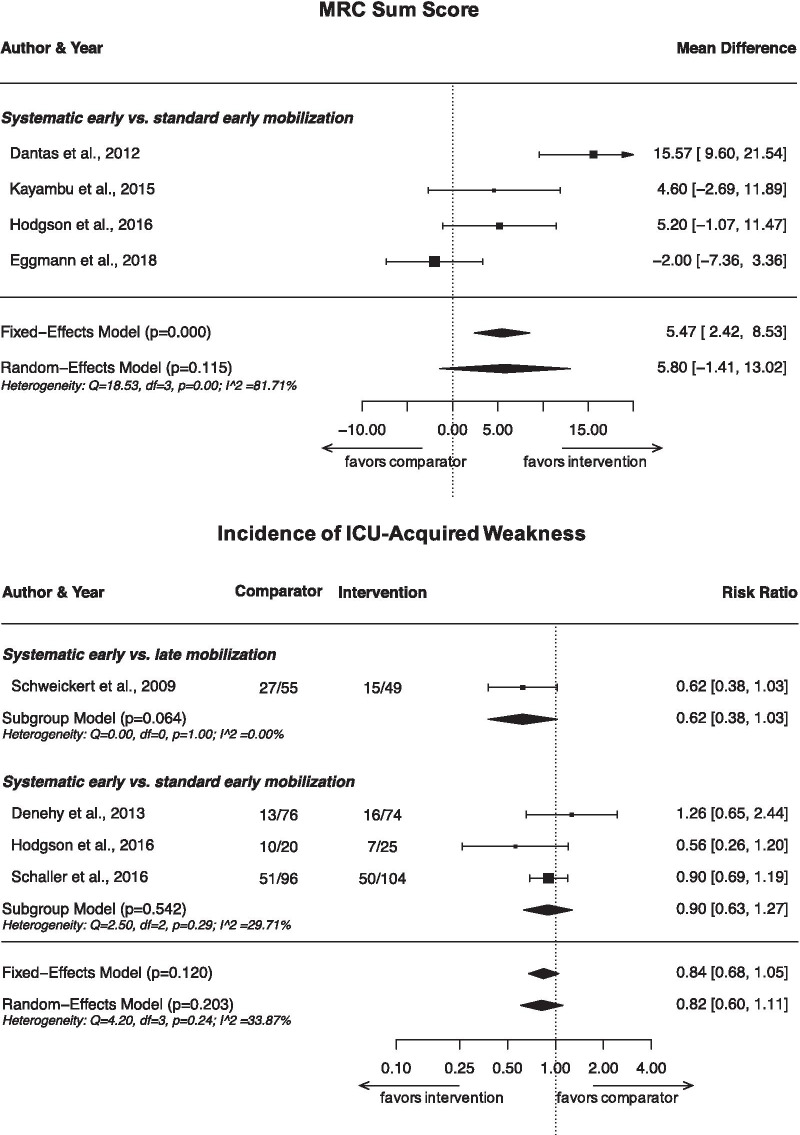
We identified 12 eligible RCTs contributing data from 1304 participants. Two RCTs were categorized as comparing systematic early with late mobilization, nine with standard early mobilization and one with no mobilization. We found evidence for a benefit of systematic early mobilization compared to late mobilization for SF-36 PFS (MD 12.3; 95% CI 3.9-20.8) and PCS (MD 3.4; 95% CI 0.01-6.8), as well as on the proportion of patients reaching independence and the time needed to walking, but not for incidence of ICUAW (RR 0.62; 95% CI 0.38-1.03) or MRC-SS. For systematic early compared to standard early mobilization, we found no statistically significant benefit on MRC-SS (MD 5.8; 95% CI - 1.4 to 13.0), incidence of ICUAW (RR 0.90; 95% CI 0.63-1.27), SF-36 PFS (MD 8.1; 95% CI - 15.3 to 31.4) or PCS (MD - 2.4; 95% CI - 6.1 to 1.3) or other priority outcomes except for change in 6MWT from baseline. Generally, effects appeared stronger for systematic early compared to late mobilization than to standard early mobilization. We judged the certainty of evidence for all outcomes as very low to low.
The evidence regarding a benefit of systematic early mobilization remained inconclusive. However, our findings indicate that the larger the difference in the timing between the intervention and the comparator, the more likely an RCT is to find a benefit for early mobilization.
PROSPERO (CRD42019122555).
本系统评价和荟萃分析旨在确定系统的早期动员在改善机械通气重症监护病房(ICU)患者的肌肉力量和身体功能方面的有效性。
我们在 MEDLINE、EMBASE 和 Cochrane 图书馆进行了两阶段系统文献检索,检索时间截至 2019 年 1 月,纳入比较早期(ICU 入住后 7 天内)与晚期、标准早期或不进行动员的随机对照试验(RCT)。主要结局为改良的医学研究理事会评分(MRC-SS)、ICU 获得性肌无力(ICUAW)发生率、6 分钟步行试验(6MWT)、达到独立行走的患者比例、行走所需时间、SF-36 生理功能评分(PFS)和 SF-36 生理健康评分(PCS)。有足够的可比证据时进行荟萃分析。我们根据 GRADE 方法评估证据的确定性。
我们确定了 12 项符合纳入标准的 RCT,共纳入 1304 名参与者。其中 2 项 RCT 比较了系统的早期与晚期动员,9 项比较了标准的早期动员,1 项比较了不进行动员。与晚期动员相比,我们发现系统的早期动员对 SF-36 PFS(MD 12.3;95%CI 3.9-20.8)和 PCS(MD 3.4;95%CI 0.01-6.8)、达到独立行走的患者比例和行走所需时间有获益,但对 ICUAW 发生率(RR 0.62;95%CI 0.38-1.03)或 MRC-SS 无获益。与标准的早期动员相比,我们发现系统的早期动员对 MRC-SS(MD 5.8;95%CI -1.4 至 13.0)、ICUAW 发生率(RR 0.90;95%CI 0.63-1.27)、SF-36 PFS(MD 8.1;95%CI -15.3 至 31.4)或 PCS(MD -2.4;95%CI -6.1 至 1.3)或其他主要结局均无统计学意义的获益,除了从基线到 6MWT 的变化。通常,与标准的早期动员相比,系统的早期动员与晚期动员相比,获益的可能性更大。我们评估所有结局的证据确定性均为极低到低。
关于系统的早期动员是否有益的证据仍不明确。但是,我们的研究结果表明,干预措施与比较组之间的时间差异越大,RCT 发现早期动员获益的可能性就越大。
PROSPERO(CRD42019122555)。