Hamano Genya, Takemura Shigekazu, Tanaka Shogo, Shinkawa Hiroji, Aota Takanori, Fujii Hiromichi, Murakami Takashi, Kuwae Yuko, Kubo Shoji
Department of Hepato-Biliary-Pancreatic Surgery, Osaka City University Graduate School of Medicine, 1-4-3 Asahimachi, Abeno-ku, Osaka, 545-8585, Japan.
Department of Cardiovascular Surgery, Osaka City University Graduate School of Medicine, 1-4-3 Asahimachi, Abeno-ku, Osaka, 545-8585, Japan.
Surg Case Rep. 2021 Jan 6;7(1):3. doi: 10.1186/s40792-020-01085-4.
Vascular invasion involving a tumor thrombus in the inferior vena cava and/or right atrium is an unfavorable prognostic factor after intrahepatic cholangiocarcinoma resection. We report an intrahepatic cholangiocarcinoma case with a tumor thrombus extending from the left hepatic vein via the inferior vena cava to the right atrium.
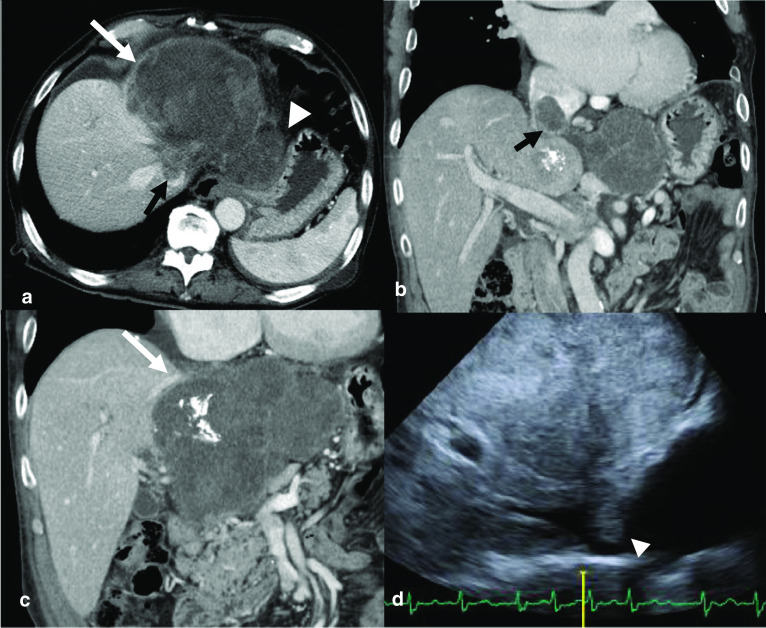
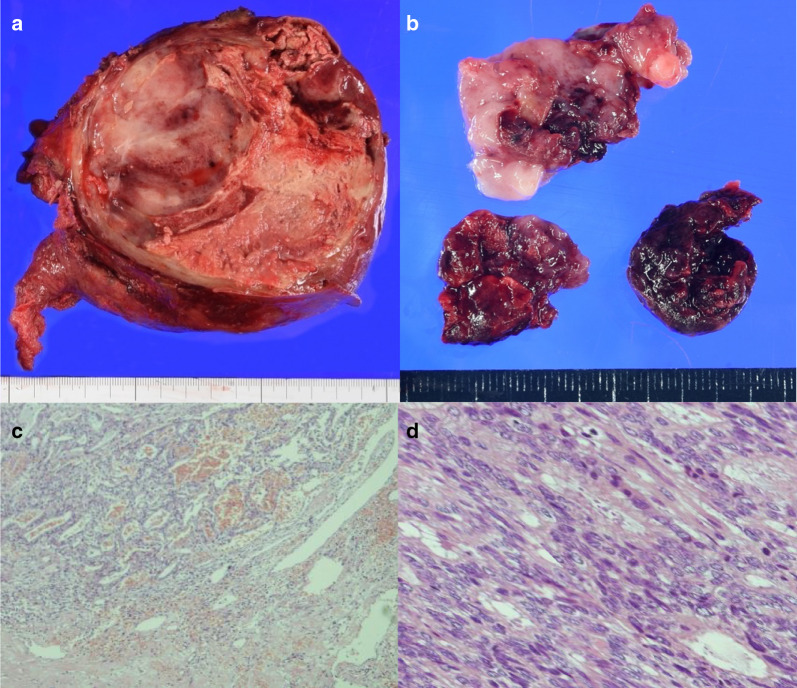
A 58-year-old man with epigastralgia was referred to our hospital after an emergent transcatheter arterial embolization was done following the radiological diagnosis of a ruptured hepatic tumor. The serum concentrations of carcinoembryonic antigen, carbohydrate 19-9, duke pancreatic monoclonal antigen type 2, and cytokeratin-19 fragments were elevated; meanwhile those of alfa-fetoprotein and des-γ-carboxy prothrombin were within normal ranges. A contrast-enhanced computed tomography scan showed a heterogeneously enhanced tumor, 13 cm in diameter, in the left lobe of the liver, enlarged lymph nodes along the lesser curvature of the stomach, and a tumor thrombus extending from the left hepatic vein via the inferior vena cava to the right atrium. We performed a left hemihepatectomy and tumor thrombectomy under total hepatic vascular exclusion to reduce the risk of sudden death. After dissection of the liver parenchyma along the left side of the middle hepatic vein, except for the left hepatic vein, the inferior vena cava just below the right atrium could be clamped by pulling down the left lobe of the liver toward the caudal side. The thrombus could be removed by incising the inferior vena cava under total hepatic vascular exclusion. Microscopic examination showed a tubular adenocarcinoma. Immunohistochemical staining was positive for cytokeratin-7, cytokeratin-19, and epithelial membrane antigen, but negative for arginase-1, glypican-3, and hepatocyte. The patient was pathologically diagnosed with an intrahepatic cholangiocarcinoma with a tumor thrombus in the inferior vena cava. Adjuvant chemotherapy with tegafur/gimeracil/oteracil was administered for 1 year. The patient remained in good health without cancer recurrence for over 4 years after the operation.
An aggressive surgical approach may be indicated for intrahepatic cholangiocarcinoma with a tumor thrombus in the inferior vena cava and/or right atrium to avoid the risk of impending death.
肝内胆管癌切除术后,血管侵犯累及下腔静脉和/或右心房内的肿瘤血栓是一个不良预后因素。我们报告一例肝内胆管癌病例,其肿瘤血栓从左肝静脉经下腔静脉延伸至右心房。
一名58岁上腹部疼痛男性,在经放射学诊断为肝肿瘤破裂后行急诊经导管动脉栓塞术,随后转诊至我院。癌胚抗原、糖类抗原19-9、杜克胰腺单克隆抗原2型和细胞角蛋白-19片段的血清浓度升高;同时,甲胎蛋白和脱γ-羧基凝血酶原在正常范围内。增强计算机断层扫描显示肝脏左叶有一个直径13厘米的不均匀强化肿瘤,胃小弯侧淋巴结肿大,以及一个从左肝静脉经下腔静脉延伸至右心房的肿瘤血栓。我们在全肝血管阻断下进行了左半肝切除术和肿瘤血栓切除术,以降低猝死风险。沿肝中静脉左侧解剖肝实质,除左肝静脉外,通过将肝左叶向尾侧下拉可夹住右心房下方的下腔静脉。在全肝血管阻断下切开下腔静脉可取出血栓。显微镜检查显示为管状腺癌。免疫组化染色细胞角蛋白-7、细胞角蛋白-19和上皮膜抗原呈阳性,但精氨酸酶-1、磷脂酰肌醇蛋白聚糖-3和肝细胞呈阴性。该患者经病理诊断为肝内胆管癌伴下腔静脉肿瘤血栓。给予替加氟/吉美嘧啶/奥替拉西辅助化疗1年。术后4年多来,患者身体健康,无癌症复发。
对于伴有下腔静脉和/或右心房肿瘤血栓的肝内胆管癌,可能需要采取积极的手术方法以避免即将死亡的风险。