Horáková Dana, Boster Aaron, Bertolotto Antonio, Freedman Mark S, Firmino Isabel, Cavalier Steven J, Jacobs Alan K, Thangavelu Karthinathan, Daizadeh Nadia, Poole Elizabeth M, Baker Darren P, Margolin David H, Ziemssen Tjalf
Department of Neurology and Center of Clinical Neuroscience, First Faculty of Medicine, Charles University and General University Hospital, Prague, Czech Republic.
The Boster Center for Multiple Sclerosis, Columbus, USA.
Mult Scler J Exp Transl Clin. 2020 Dec 18;6(4):2055217320972137. doi: 10.1177/2055217320972137. eCollection 2020 Oct-Dec.
Few data exist concerning conversion to secondary progressive MS in patients treated with disease-modifying therapies.
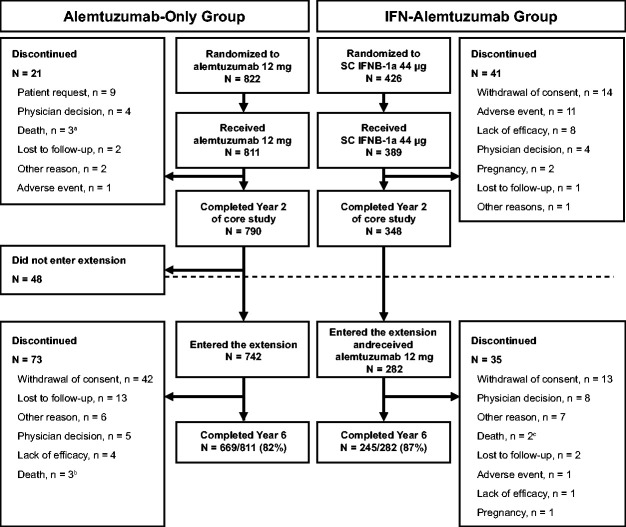
Determine the proportion of alemtuzumab-treated patients converting from relapsing-remitting to secondary progressive MS during the CARE-MS core and extension studies.
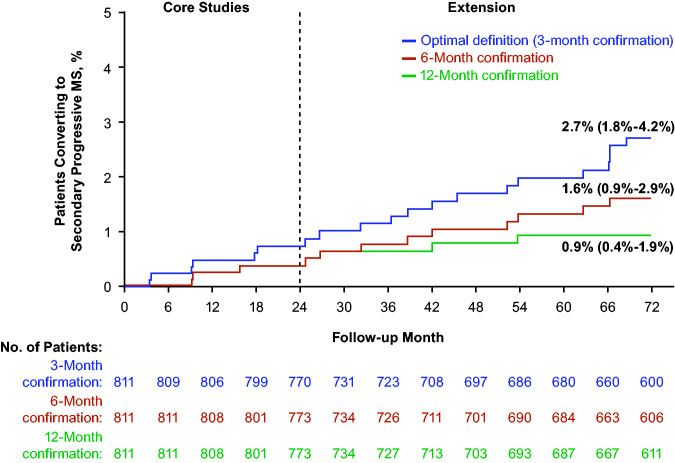
Patients ( = 811) were analyzed post hoc for secondary progressive MS conversion. Optimal conversion definition: Expanded Disability Status Scale (EDSS) score ≥4, pyramidal functional system score ≥2, and confirmed progression over ≥3 months including confirmation within the functional system leading to progression, independent of relapse.
Over 6.2 years median follow-up, 20 alemtuzumab-treated patients converted (Kaplan-Meier estimate, 2.7%; 95% confidence interval, 1.8%-4.2%). Sensitivity analysis accounting for dropouts showed similar results (3%), as did analyses using alternative definitions with different EDSS thresholds and/or confirmation periods, and analysis of core study subcutaneous interferon beta-1a-treated patients who received alemtuzumab in the extension. Patients converting to secondary progressive MS were older, and had higher EDSS scores and greater brain lesion volumes at baseline, but did not need additional alemtuzumab or other therapies.
The 6-year conversion rate to secondary progressive MS was low for alemtuzumab-treated patients, supporting further study of the role alemtuzumab may play in reducing risk of secondary progression. NCT00530348, NCT00548405, NCT00930553.
关于接受疾病修饰疗法的患者转化为继发进展型多发性硬化症的数据很少。
确定在CARE-MS核心研究和扩展研究中,接受阿仑单抗治疗的患者从复发缓解型转化为继发进展型多发性硬化症的比例。
对811例患者进行事后分析,以确定继发进展型多发性硬化症的转化情况。最佳转化定义:扩展残疾状态量表(EDSS)评分≥4,锥体功能系统评分≥2,且在≥3个月内确认病情进展,包括在导致病情进展的功能系统内得到确认,与复发无关。
在6.2年的中位随访期内,20例接受阿仑单抗治疗的患者发生了转化(Kaplan-Meier估计值为2.7%;95%置信区间为1.8%-4.2%)。对失访情况进行敏感性分析得到了相似结果(3%),使用不同EDSS阈值和/或确认期的替代定义进行分析,以及对在扩展研究中接受阿仑单抗治疗的核心研究中皮下注射干扰素β-1a的患者进行分析,结果也是如此。转化为继发进展型多发性硬化症的患者年龄较大,基线时EDSS评分较高,脑病变体积较大,但不需要额外的阿仑单抗或其他治疗。
接受阿仑单抗治疗的患者转化为继发进展型多发性硬化症的6年转化率较低,这支持进一步研究阿仑单抗在降低继发进展风险中可能发挥的作用。临床试验注册号:NCT00530348、NCT00548405、NCT00930553。